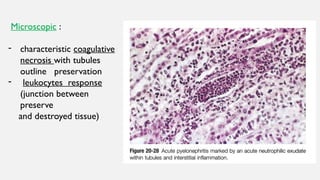
1. Acute pyelonephritis is a bacterial infection of the kidney that is usually associated with a urinary tract infection. It is characterized microscopically by patchy inflammation, neutrophils in the tubules, and tubular necrosis.
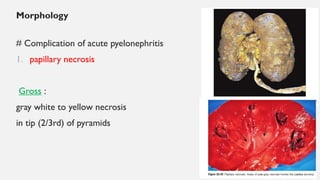
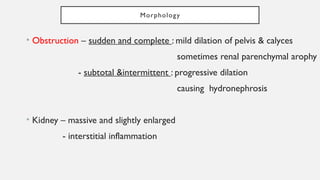
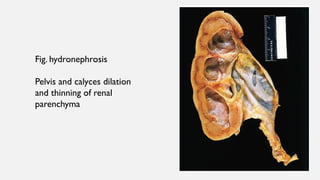
2. Complications of acute pyelonephritis include papillary necrosis, pyonephrosis, and perinephric abscess. Hydronephrosis is dilation of the renal pelvis and calyces due to urinary outflow obstruction.
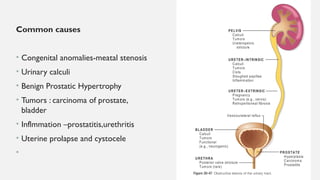
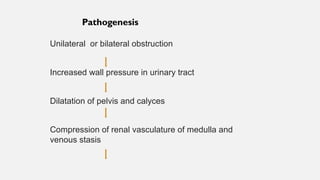
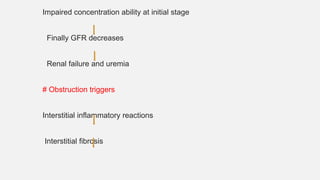
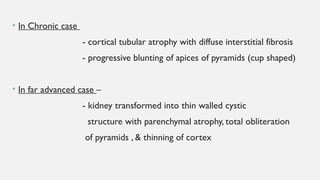
3. Hydronephrosis is caused by various congenital and acquired conditions and can lead to impaired kidney function, fibrosis, and end-stage renal atrophy if long-standing and complete