Downloaded 201 times


























The document discusses hydronephrosis and pyonephrosis, detailing their definitions, causes, pathophysiology, clinical features, investigations, and treatment options. Hydronephrosis is characterized by the dilatation of kidney structures due to urinary obstruction, while pyonephrosis refers to the infection that follows hydronephrosis. Treatment varies based on the underlying cause and includes both medical management and surgical intervention when necessary.
Introduction to Hydronephrosis and Pyonephrosis, including contents overview.
Hydronephrosis is aseptic dilatation of the kidney due to obstruction affecting urine outflow.
Causes including extramural, intramural, and intraluminal obstructions leading to unilateral hydronephrosis.
Bilateral hydronephrosis primarily results from urethral obstruction, with congenital and acquired causes.
Effects of obstruction on renal function, time-dependent changes leading to kidney damage.
Signs of unilateral and bilateral hydronephrosis, including renal symptoms and post-obstructive diuresis.
Possible examination findings and various investigative methods such as ultrasound and pyelography.
Management approaches based on severity including surgical and medical treatments for hydronephrosis.
Surgical techniques like Anderson-Hynes pyeloplasty and endoscopic pyeloplasty for hydroureter.
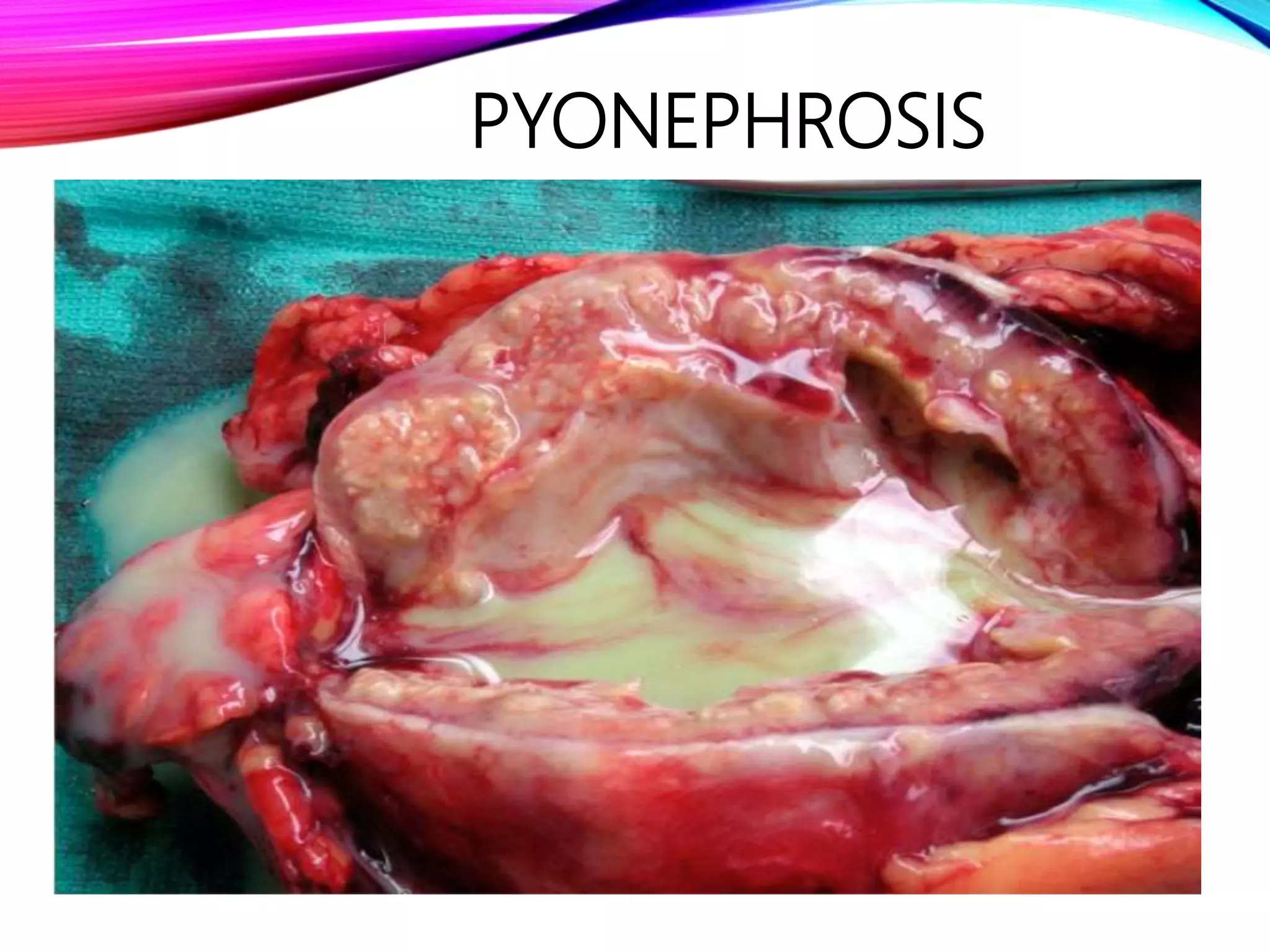
Definition and causes of Pyonephrosis, an infection often following hydronephrosis.
Triad symptoms of pyonephrosis including fever, anemia, and loin swelling.
Investigation findings pointing to the presence of calculus and pus-filled collecting system.
Emergency treatment protocols including antibiotics and possible nephrectomy in severe cases.
List of references used for the presentation, covering key urology textbooks.























































































