Downloaded 162 times
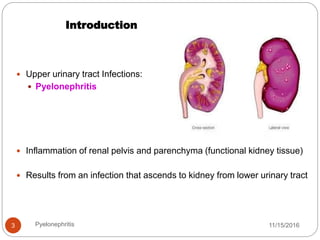
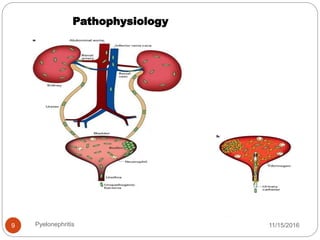
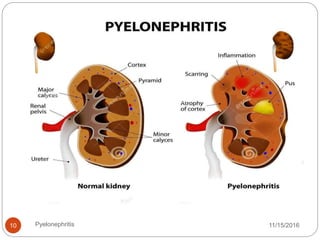
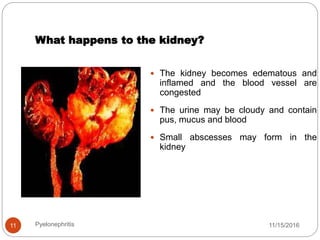
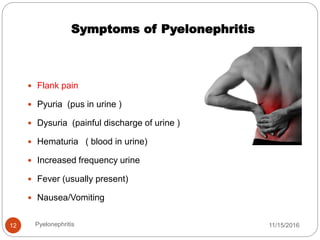
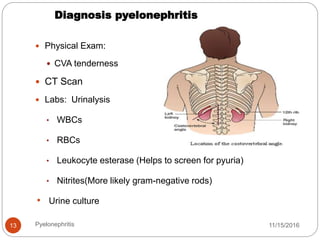

Pyelonephritis is an infection and inflammation of the kidneys that is usually caused by bacteria ascending from the lower urinary tract. It is more common in females than males, especially between ages 15-35. Common symptoms include flank pain, fever, nausea, and urinary symptoms like dysuria and hematuria. Diagnosis involves urinalysis showing white blood cells and a urine culture. Treatment focuses on antibiotics and prevention emphasizes frequent urination and hydration to maintain bladder health.






















































































![谷歌留痕技术 [ 𝙩𝙤𝙥 𝟮𝟯𝟯. 𝙘 𝙤𝙢 ]](https://cdn.slidesharecdn.com/ss_thumbnails/top233-260130174328-3833018c-thumbnail.jpg?width=640&height=640&fit=bounds)









