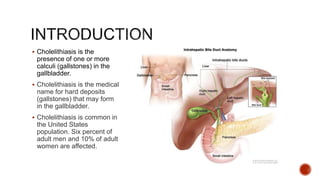
Cholelithiasis is the presence of gallstones in the gallbladder, affecting 6% of adult men and 10% of adult women in the U.S. These stones form due to bile supersaturation with cholesterol, excessive bilirubin, or improper gallbladder emptying, leading to symptoms such as abdominal pain, jaundice, and digestive issues. Management includes medical treatments, surgical options like cholecystectomy, and post-operative care assessments to prevent complications.