Downloaded 404 times











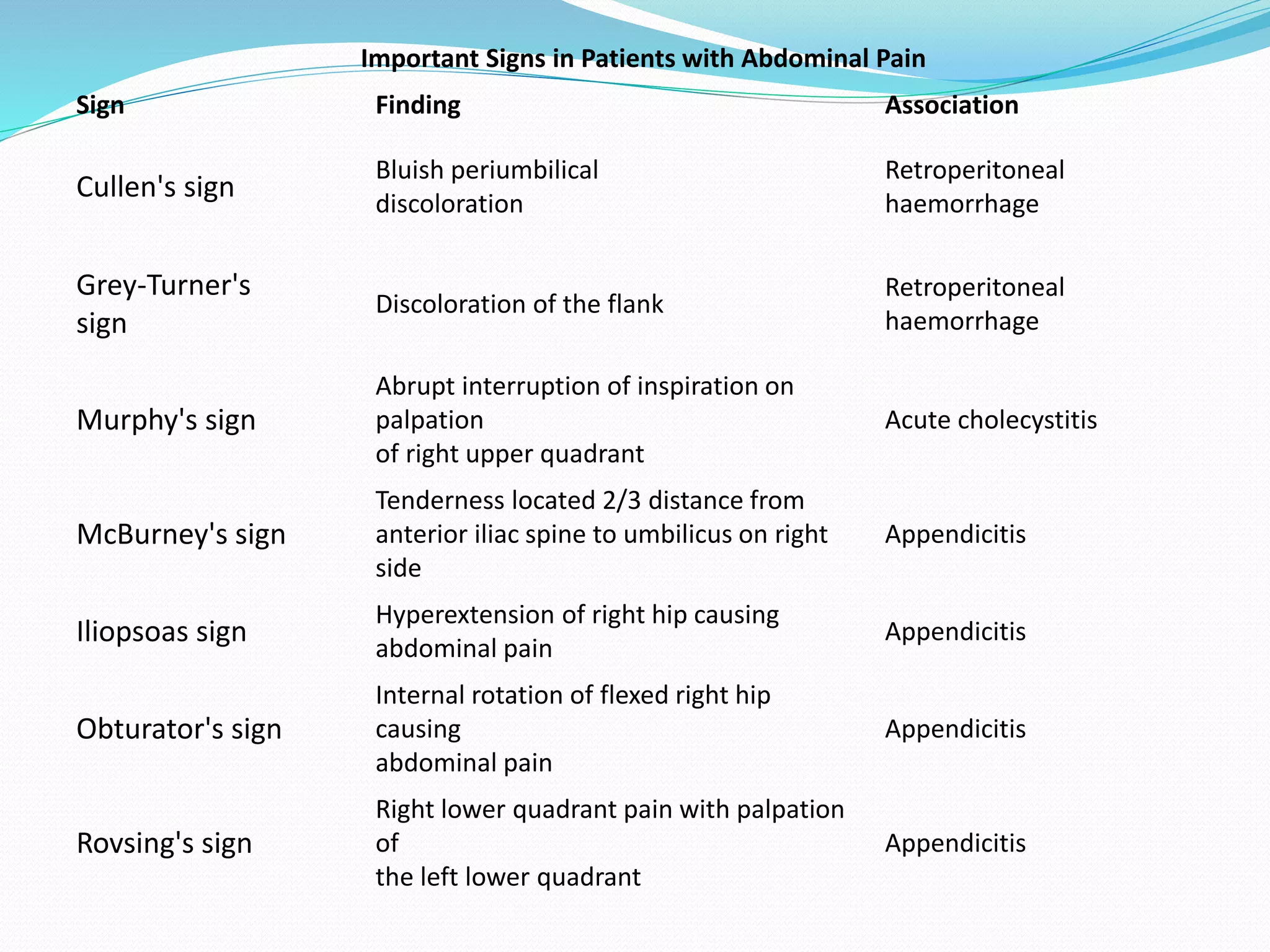





























This document outlines a presentation on the pathophysiology and management of acute abdomen. It begins with definitions of acute abdomen and types of abdominal pain. Pathophysiological mechanisms including luminal obstruction, inflammation, peritonitis, ischemia and non-specific pain are described. Common causes like appendicitis, cholecystitis, bowel obstruction and perforated viscus are listed. Immediately life-threatening diagnoses of perforated viscus, bowel ischemia, ruptured abdominal aortic aneurysm and ruptured ectopic pregnancy are highlighted. Clinical assessment techniques and investigations are outlined. Management principles focusing on ABCs, fluid resuscitation and need for surgery in some cases are emphasized in the take-home message.











































































































