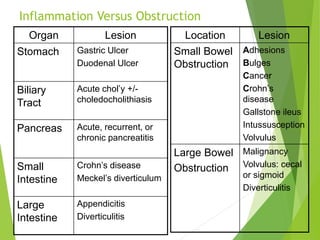
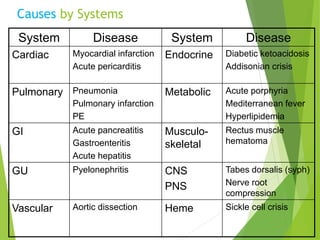
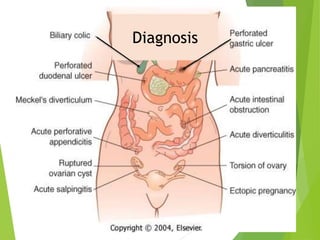
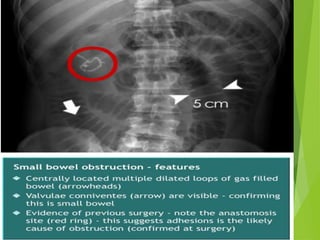
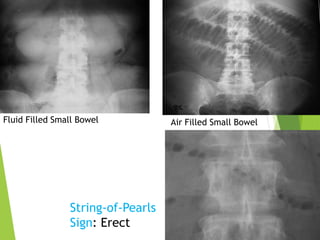
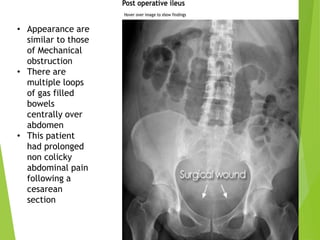
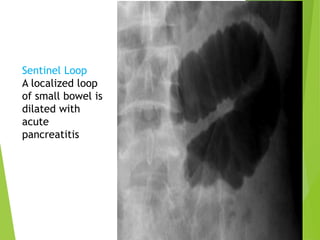
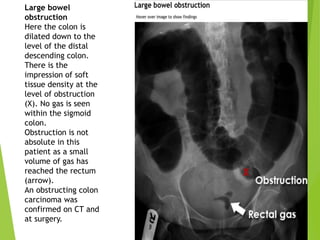
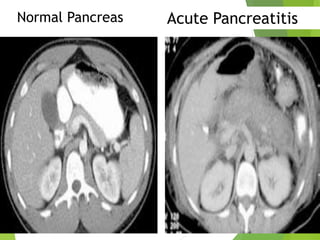
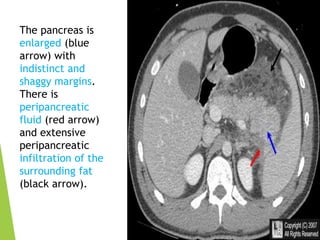
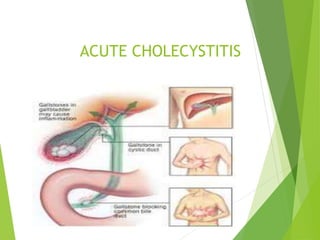
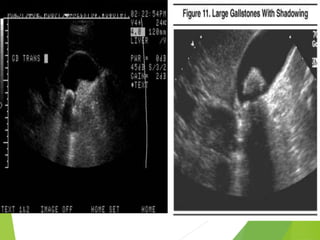
This document provides an overview of various acute abdominal conditions, including their causes, locations, and diagnostic findings. It covers inflammation versus obstruction, diseases of the stomach, biliary tract, pancreas, small intestine, and large intestine. Specific conditions summarized include acute appendicitis, acute pancreatitis, acute cholecystitis, small bowel obstruction, large bowel obstruction such as volvulus, and pneumoperitoneum. Imaging findings on x-ray, ultrasound, CT, and signs such as Rigler's sign are described for diagnosing these acute abdominal conditions.