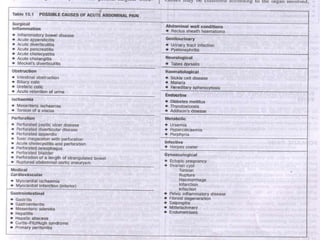
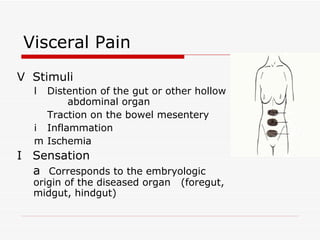
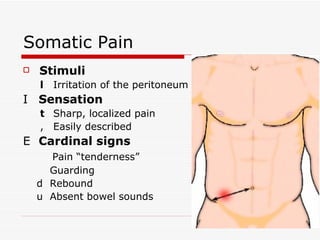
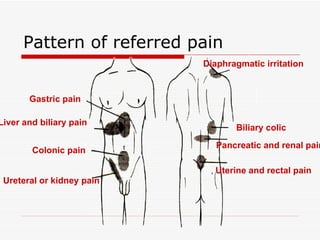
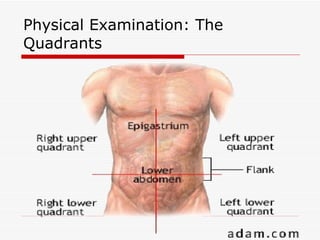
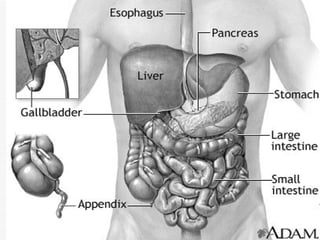
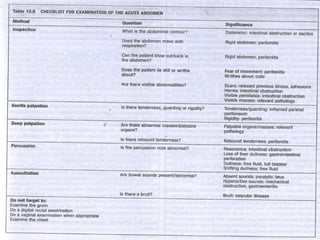
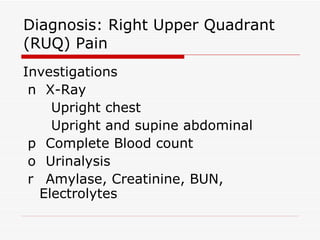
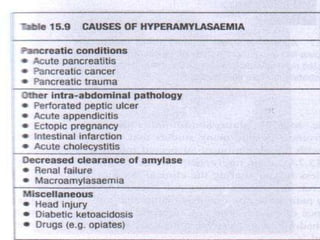
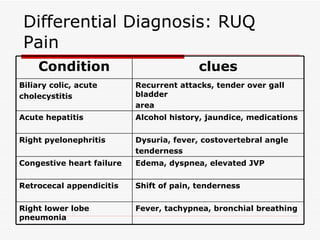
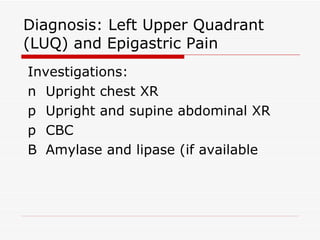
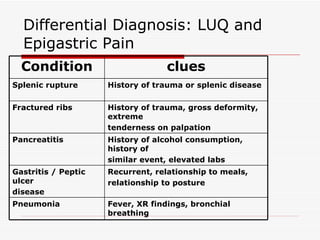
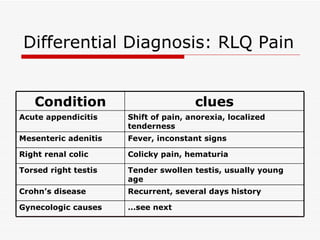
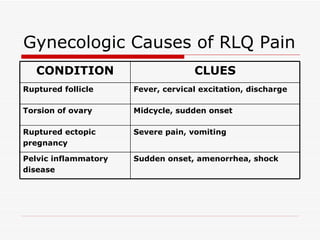
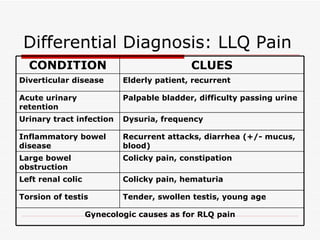
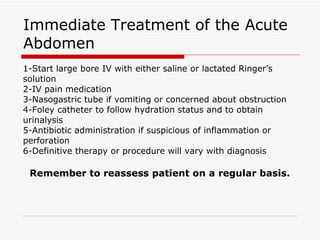
The document discusses the acute abdomen, which refers to intra-abdominal disease that is often best treated surgically. It outlines characteristics of patients who need surgery versus those who do not, and provides potential non-surgical and metabolic causes of acute abdominal pain. The physiology of abdominal pain and patterns of referred pain are described. A history and physical exam are important for diagnosis, with differential diagnoses provided for various locations of abdominal pain. Immediate treatment of the acute abdomen includes IV fluids, pain medication, tubes, antibiotics, and definitive therapy based on diagnosis.