Downloaded 76 times
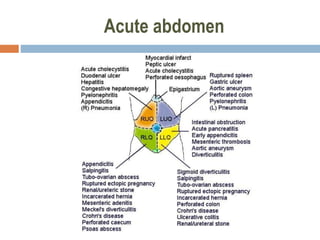


This document discusses acute abdomen, including causes, symptoms, and examination findings. It notes that acute abdomen involves sudden severe abdominal pain that may be life-threatening. Common intra-abdominal causes include inflammation, perforation, obstruction, and hemorrhage. Examination involves inspection, palpation, percussion, and auscultation of the abdomen, as well as relevant history and lab/imaging tests. Imaging tests like x-ray, ultrasound, and CT scan can help identify conditions like perforation, obstruction, or masses.



































































