Downloaded 125 times


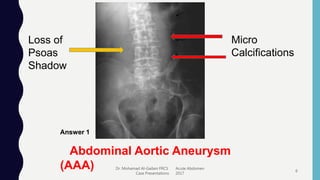
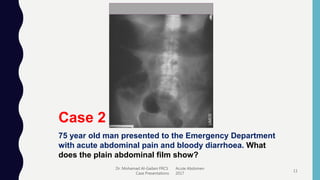
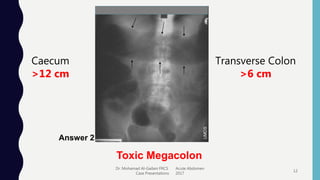
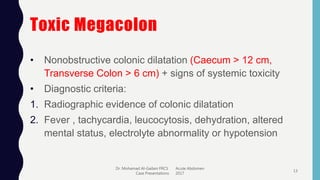

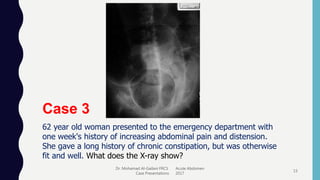
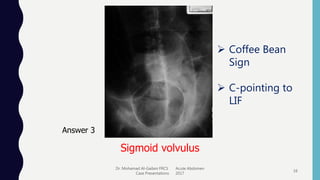

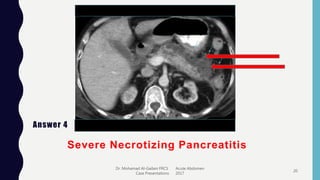
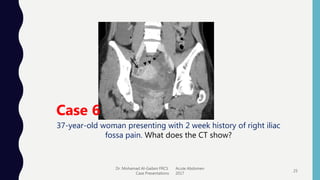
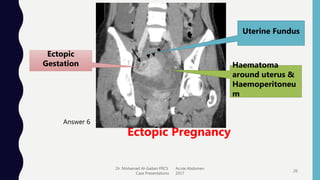
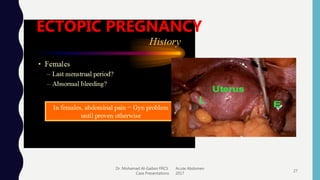


The document presents case studies on acute abdomen, highlighting its urgency and the importance of timely diagnosis and management. It discusses various conditions associated with acute abdomen, such as abdominal aortic aneurysm, toxic megacolon, sigmoid volvulus, and ectopic pregnancy, detailing symptoms, diagnostic imaging, and treatment approaches. Key takeaways include the need for rapid evaluation, pre-operative optimization, and considerations for surgical intervention.


























![[MBBS/MS/DNB] Sample EXAM Long Case on Breast Lump](https://cdn.slidesharecdn.com/ss_thumbnails/cccbreast-200518145117-thumbnail.jpg?width=640&height=640&fit=bounds)








































































