Downloaded 65 times
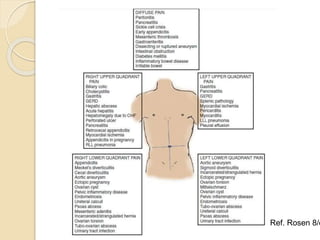
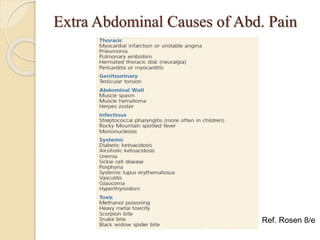


The document outlines the approach to diagnosing and managing acute abdomen pain, detailing three pain pathways: visceral, somatic, and referred. It emphasizes the importance of a quick assessment using the SAMPLE method and suggests several examination techniques, as well as early interventions such as pain management and imaging modalities. The document also highlights the need for proper disposition from the emergency department based on diagnosis, particularly for patients with non-specific abdominal pain.






































































































