Download as PPS, PPTX







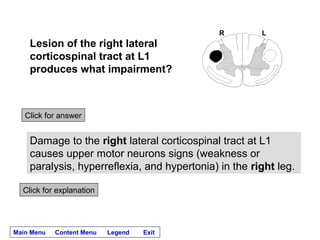





















The patient is unable to stand or walk because he is unable to move or bear weight on his right leg. On examination: - Strength is normal in the left leg but there is weakness of dorsiflexion and plantarflexion in the right leg. - Reflexes are normal in the left leg but hyperreflexic in the right leg. - Sensation to light touch, pinprick and temperature are intact throughout. - There is spasticity in the right leg. Damage to what system(s) is causing this patient’s problems? Lesion of the right lateral corticospinal tract at approximately L2. The findings are consistent with an













































































