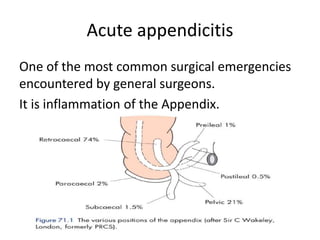
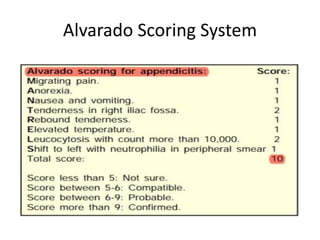
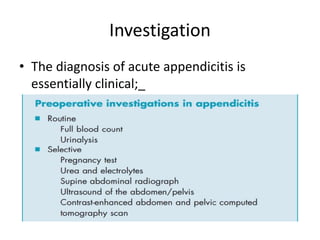
Acute abdomen and appendicitis are medical emergencies that require prompt diagnosis and treatment. The document discusses the clinical presentation of acute abdomen, with a focus on acute appendicitis. Key signs of acute appendicitis include abdominal pain that starts around the umbilicus and later localized to the right lower quadrant, as well as nausea, vomiting, fever and rebound tenderness on physical exam. A diagnosis is typically made clinically based on history and exam findings, supported by blood tests and imaging as needed. Treatment involves surgical removal of the appendix (appendectomy), most often via laparoscopy. Delays in diagnosis and treatment can lead to complications from appendicitis.