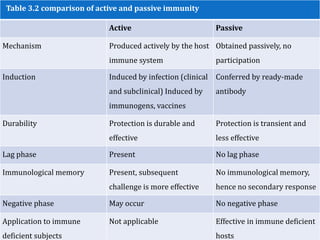
This document discusses different types of immunity, including active and passive immunity. It provides details on active immunity, such as how it is acquired through exposure to antigens and produces a lasting immune response. Passive immunity is described as obtaining resistance through introduction of ready-made antibodies rather than active immune response. Local immunity focuses on mucosal surfaces and secretory IgA. Examples of natural and artificial acquisition of both active and passive immunity are also outlined.