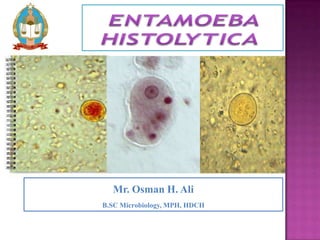
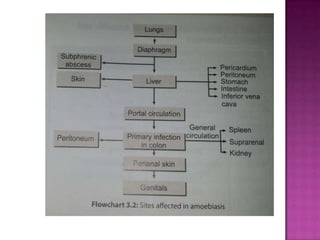
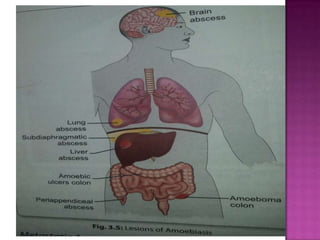
This document summarizes Entamoeba histolytica, an intestinal parasite. It discusses the morphology and life cycle of E. histolytica, including its trophozoite and cyst forms. It describes the pathogenesis of intestinal and extra-intestinal amoebiasis caused by E. histolytica, affecting the colon, liver, lungs and other organs. Clinical features include amoebic dysentery and liver abscesses. Laboratory diagnosis and treatment options are also mentioned. Prevention focuses on avoiding contaminated food/water and treating asymptomatic cyst carriers.