4th ventricle 21.12.2015.dk.
•
78 likes•8,387 views

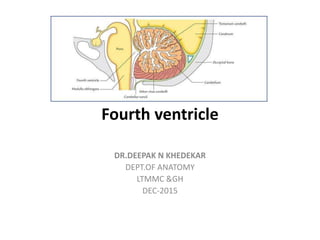
The fourth ventricle is located in the posterior cranial fossa between the cerebellum and brainstem. It has five recesses and communicates with the cerebral aqueduct and central canal of the medulla. The roof is formed by the superior cerebellar peduncles and medullary velum, which contains the choroid plexus. The floor is rhomboid-shaped and formed by the pons and medulla, containing important nuclei. The fourth ventricle plays a role in circulation of cerebrospinal fluid and can be affected in conditions like medulloblastoma and hydrocephalus.

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (18)
Similar to 4th ventricle 21.12.2015.dk.
Similar to 4th ventricle 21.12.2015.dk. (20)
More from Deepak Khedekar
More from Deepak Khedekar (20)
Recently uploaded
Recently uploaded (20)
4th ventricle 21.12.2015.dk.
- 1. Fourth ventricle DR.DEEPAK N KHEDEKAR DEPT.OF ANATOMY LTMMC &GH DEC-2015
- 2. Introduction… • Brain develops from the enlarged cranial part of the neural tube. • At the end of 4th week, the enlarged cephalic part shows 3 distinct dilatations- Primary brain vesicles. • Cavities of vesicles form the ventricular system of the adult brain.
- 4. Primary brain vesicles . • Craniocaudally, these are: Prosencephalon (forebrain) Mesencephalon (mid-brain) Rhombencephalon (hindbrain).
- 7. Cerebrospinal Fluid • Cerebrospinal fluid (CSF) is similar to that of blood plasma and interstitial fluid. • Present in the ventricular system within the CNS and in the subarachnoid space surrounding the CNS. • Bathes both the external and internal surfaces of the brain and spinal cord . • Provides a protective cushion between the CNS and the surrounding bones. • In an adult, the total volume of CSF is about 150 ml, out of which only 30 ml is in the ventricular system and remainder in the subarachnoid space.
- 10. Introduction… • Tent-like cavity of hindbrain. • Site- Posterior cranial fossa • Location- Cerebellum in front. Pons and upper part of medulla oblongata behind. • Lined with ependyma and filled with CSF
- 13. Introduction…
- 14. Introduction… Cavity of the ventricle presents- Triangular outline in sagittal section and Rhomboidal in shape (lozenge-shaped) in horizontal section. • Continuous with… Cerebral aqueduct of midbrain. Central canal of medulla oblongata
- 15. 4th ventricle
- 16. 4th ventricle • Recesses • Angles • Openings • Floor • Roof • Applied anatomy
- 17. 1.Recesses… • 5 in no. • Extensions from the cavity. 2- lateral recesses 1- median dorsal recess 2- lateral dorsal recesses
- 18. Lateral Recesses • One on each side, lies in the interval between… Inferior cerebellar peduncle ventrally Peduncle of flocculus dorsally. • Lateral extremity reaches up to the flocculus • Opens into the subarachnoid space of cerebellopontine angle (CP angle) as the lateral aperture (foramen of Luschka) through which part of choroid plexus bulges out.
- 19. 1.Recesses…
- 20. 1.Recesses… Median dorsal recess- • Extends into the white core of the cerebellum • Lies just above (cranial) to the nodule. Two lateral dorsal recesses- • One on each side of median dorsal recess • Project dorsally above the inferior medullary velum • Lies immediately lateral to the nodule.
- 21. 2.Angles • 4 angles Superior - is continuous above with the cerebral aqueduct of midbrain. Inferior - is continuous below with the central canal of the closed part of the medulla oblongata. 2 lateral - one on each side is carried outwards across the dorsal surface of the inferior cerebellar peduncle as tubular pouches called lateral recess.
- 22. 3.Boundaries of the fourth ventricle
- 23. 4.Roof (posterior wall) • Tent-shaped,has upper and lower sloping surfaces. • Apex of the tent extends posteriorly into the white core of the cerebellum. • Upper part of the roof is formed by the convergence of two Superior cerebellar peduncles and a thin sheet of white mater bridging it.
- 24. Medullary velum • Bridges the triangular gap between the two cerebellar peduncles
- 25. Superior medullary velum • Bridges the triangular gap between the two superior cerebellar peduncles Inferior medullary velum • formed conjointly by the ventricular ependyma and the pia mater (of tela choroidea)
- 26. 4.Roof… Lower part is formed by… Inferior medullary velum a thin sheet of non-nervous tissue, the that covers it posteriorly. • intimately related to the nodule of the inferior vermis of the cerebellum.
- 27. 4.Roof… Foramen of Magendie – • Large aperture in the median plane in lower part of the inferior medullary velum • Through which the cavity of fourth ventricle communicates with the subarachnoid space of the cerebellomedullary cistern (cisterna magna).
- 28. Tela choroidea • Double layered fold of pia mater • Lies between the inferior vermis of the cerebellum and lower part of the roof of the fourth ventricle. • Layers- 1.Dorsal layer- • lines the inferior vermis which on reaching the nodule • is reflected upon itself to form its ventral layer. • When traced laterally, the dorsal layer is continuous with the pia mater covering the cerebellar hemisphere.
- 29. Tela choroidea 2.Ventral layer- • lies over the roof of lower part of fourth ventricle • continuous with the pia mater covering the dorsal aspect of medulla oblongata
- 30. Choroid plexuses • Formed by capillary plexus of blood vessels between the two layers of tela choroidea . • Form the rich vascular fringe that projects through the lower part of the roof of the fourth ventricle to form the choroid plexus. • Derived from the branches of posterior inferior cerebellar arteries.PICA
- 31. Choroid plexus • T’-shaped plx • projects into the cavity through the lower part of the roof. • Vertical limb of ‘T’- is double with foramen of Magendie intervening between the two limbs. • Horizontal limb -on either side extends into the lateral recess, protrudes through the lateral aperture, foramen of Luschka • Can be seen on the surface of brain, near the flocculus.
- 32. 5.Floor (rhomboid fossa) Formed by… Posterior surfaces of the pons Upper part of the medulla. • Rhomboid in shape (diamond-shaped) • Divisible into 3 parts
- 33. 5.Floor Divisible into… 1.Upper part: is formed by the posterior surface of the pons. 2. lower triangular part: is formed by the upper part of the posterior surface of the medulla.
- 34. 5.Floor… 3.Intermediate part : • At the junction of the medulla and pons • Prolonged laterally on either side over the inferior cerebellar peduncle as the floor of lateral recess. • Bounded above by base of upper triangular part of the floor and below by a line joining the horizontal parts of the taenia. • Surface of intermediate part is marked by the presence of delicate bundles of transversely arranged fibres, the striae medullaris.
- 35. 5.Floor…
- 36. 5.Floor • Median sulcus – divides floor into right and left symmetrical halves. • Medial eminence- longitudinal elevation on either side of median sulcus • Medial eminence is bounded laterally by sulcus limitans. • Vestibular area- lateral to sulcus limitans, containing vestibular nuclei. • Vestibular area lies partly in the pons and partly in the medulla oblongata. • Superior fovea – widen triangular depression at the upper end of sulcus limitans
- 37. 5.Floor…
- 38. Locus ceruleus • Bluish grey area lies above the superior fovea where the sulcus limitans flattens out • Colour is imparted by the underlying group of nerve cells containing melanin pigment which constitute the substantia ferruginea. • Neurons of locus ceruleus contain large quantities of norepinephrine (noradrenaline).
- 39. Inferior fovea. • lowermost part of sulcus limitans presents a small depression Facial colliculus • An oval swelling present on either side, the medial eminence in the pontine part of floor at the level of superior fovea. • Swelling is produced by the fibres from the motor nucleus of facial nerve hooking around the abducent nucleus (internal genu of facial nerve).
- 40. Medullary part of the floor • From inferior fovea the sulcus limitans descends obliquely towards the median sulcus. • Sulcus divides the medial eminence in the into two triangles - Hypoglossal triangle above Vagal triangle below.
- 41. Floor-Hypoglossal triangle Divided by a faint oblique furrow into… • Medial part which overlies the nucleus of hypoglossal nerve • lateral part overlying the nucleus intercalatus.
- 42. Floor-Intercalated nucleus • Described by Rutilio staderini in 1894, Italian neuroanatomist,also called as Staderini nucleus • is a group of nerve cells in the medulla oblongata, between the dorsal nucleus of vagus nerve(lateral to it ) and the nucleus of hypoglossal nerve (medial to it). • Forming part of the Perihypoglossal nuclear complex. • Probably involved in the control of the vestibulo- ocular reflex. • May contribute to the vertical neural integrator.
- 43. Floor-Vagal triangle • Overlies the nuclei of vagus, glossopha- ryngeal and cranial accessory nerves. • Crossed by a narrow translucent ridge called funiculus separans.
- 44. Area Postrema… • Small area between the funiculus separans above and the gracile tubercle below. • consists of highly vascular neuroglial tissue.
- 45. • Taenia-Infero-lateral margins of the fourth ventricle are marked by a narrow white ridge • Two taenia meet at the inferior angle of the ventricle to form a small fold called obex. • Obex-roof of the inferior angle of the fourth ventricle.
- 46. 6.Openings • 5 openings -through which cerebrospinal fluid can leave the cavity of 4th ventricle: Central aperture in the roof (f.of Magendie) Two lateral apertures in the roof (f.of Luschka). Central canal of medulla oblongata. Cerebral aqueduct of midbrain.
- 47. 7.Applied anatomy… • Medullablastoma: • Most common tumour in this region , mostly in children. • Arises from poorly differentiated primitive neuroectodermal cells of cerebellar vermis and occur. • highly malignant and produces the signs and • symptoms of cerebellar lesions, or it may press upon the vital centres located beneath the floor of the ventricle causing cardiac irregularities, tachycardia, irregular respiration, and vasomotor disturbances.
- 48. Hydrocephalus • is an abnormal increase in the volume of the cerebrospinal fluid within the skull. • If the hydrocephalus is accompanied by a raised cerebrospinal fluid pressure, then it is due to one of the following: (1) an abnormal increase in the formation of the fluid,(2) a blockage of the circulation of the fluid, or (3) a diminished absorption of the fluid. • Rarely, hydrocephalus occurs with a normal cerebrospinal fluid pressure, and in these patients, there is a compensatory hypoplasia or atrophy of the brain substance.
- 49. Thank You