
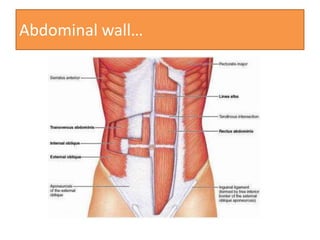









This document provides an overview of clinical anatomy of the abdomen. It discusses various abdominal structures including the abdominal wall, hernias, the liver, spleen, pancreas, intestines, and vasculature. Common abdominal conditions are described such as ulcers, appendicitis, cirrhosis, portal hypertension, and abdominal aortic aneurysm. Surgical procedures addressed include cholecystectomy, splenectomy, colectomy, and lithotripsy.





























































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)











