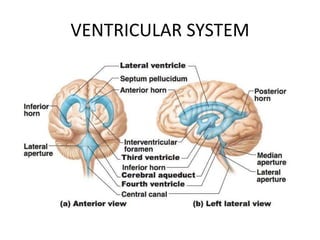
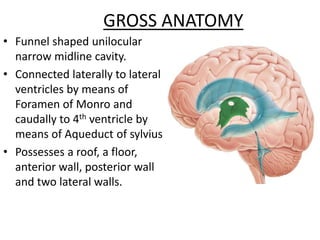
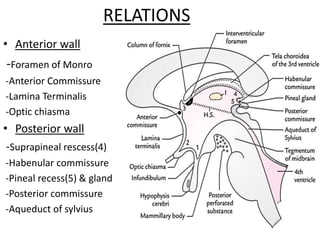
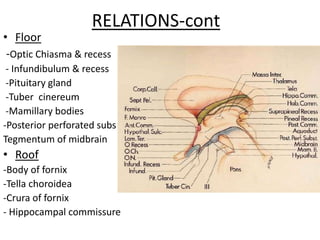
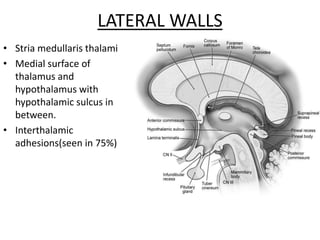
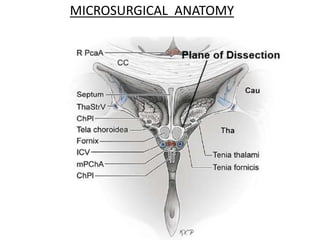
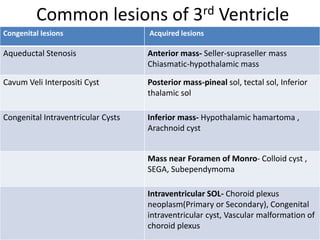
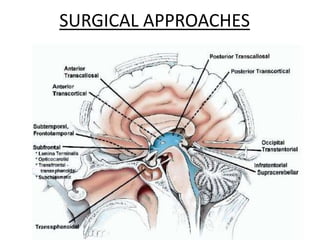
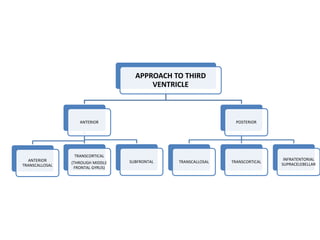
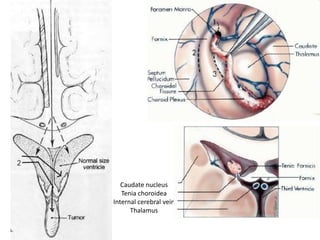
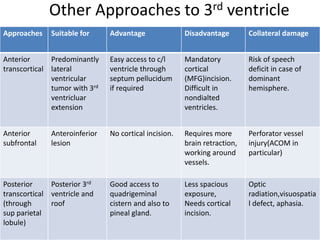
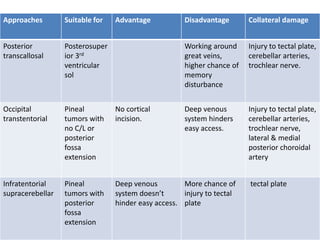
The document discusses the surgical anatomy of the third ventricle, highlighting its complex structure and relation to surrounding neural elements, which presents challenges for access during interventions. It describes the anatomical features, including walls and connections to neighboring ventricles, as well as common lesions and various surgical approaches with their respective advantages and disadvantages. Specific concerns regarding possible collateral damage to critical structures during approaches to the third ventricle are also noted.

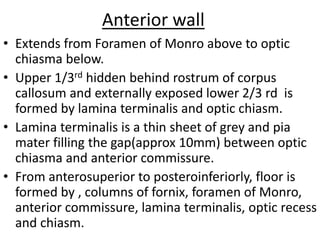







































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)















