Downloaded 470 times

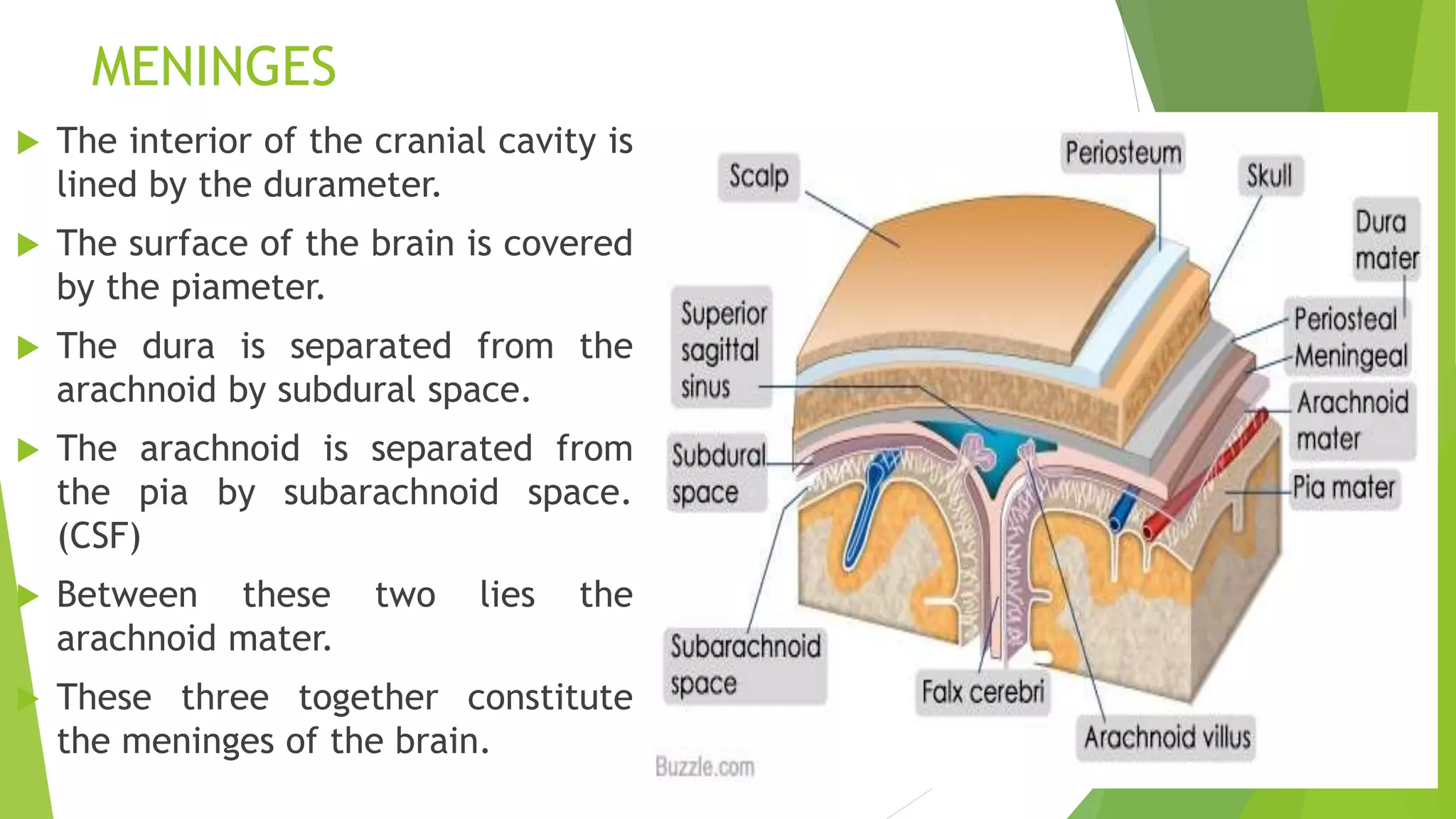
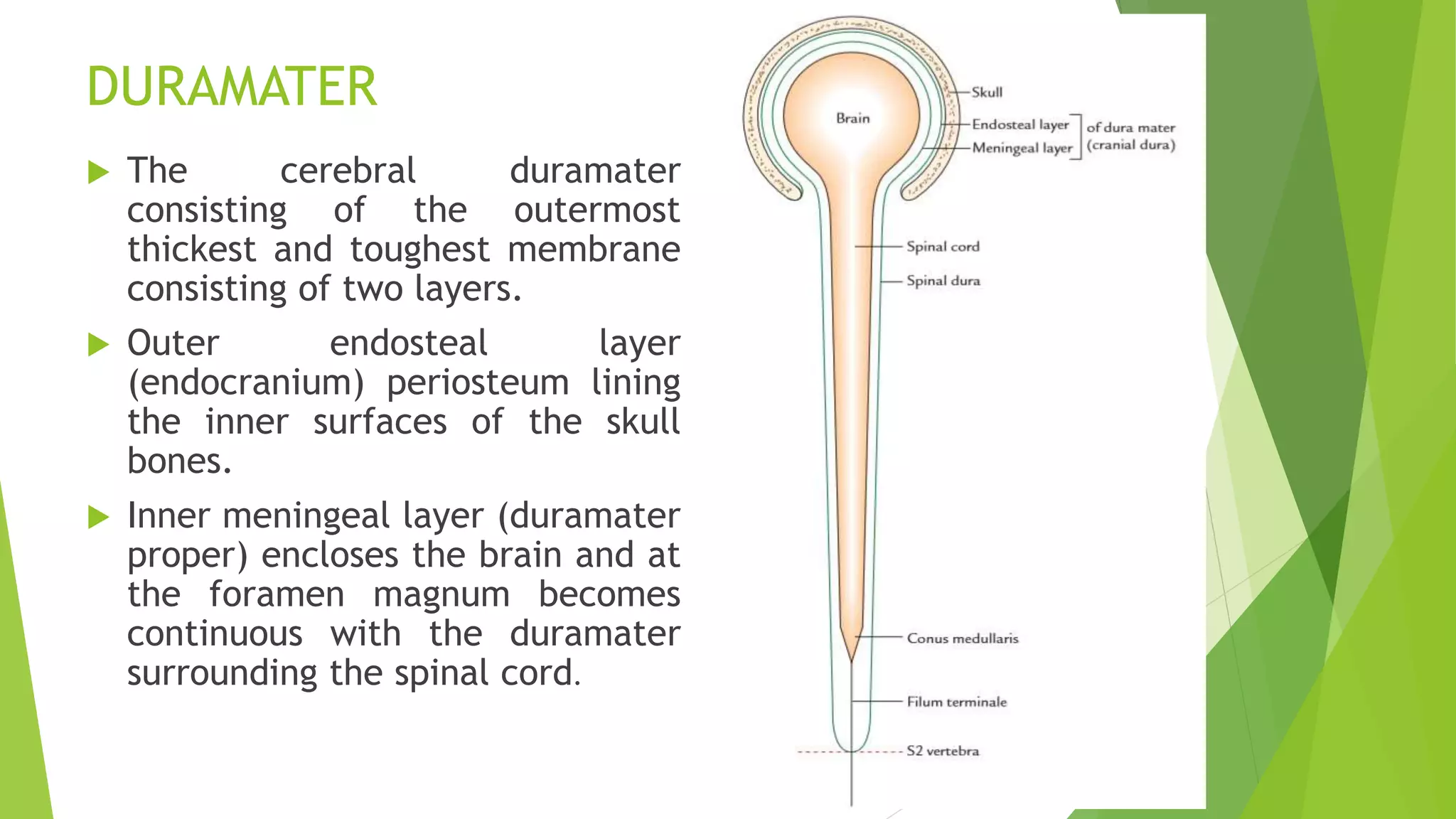
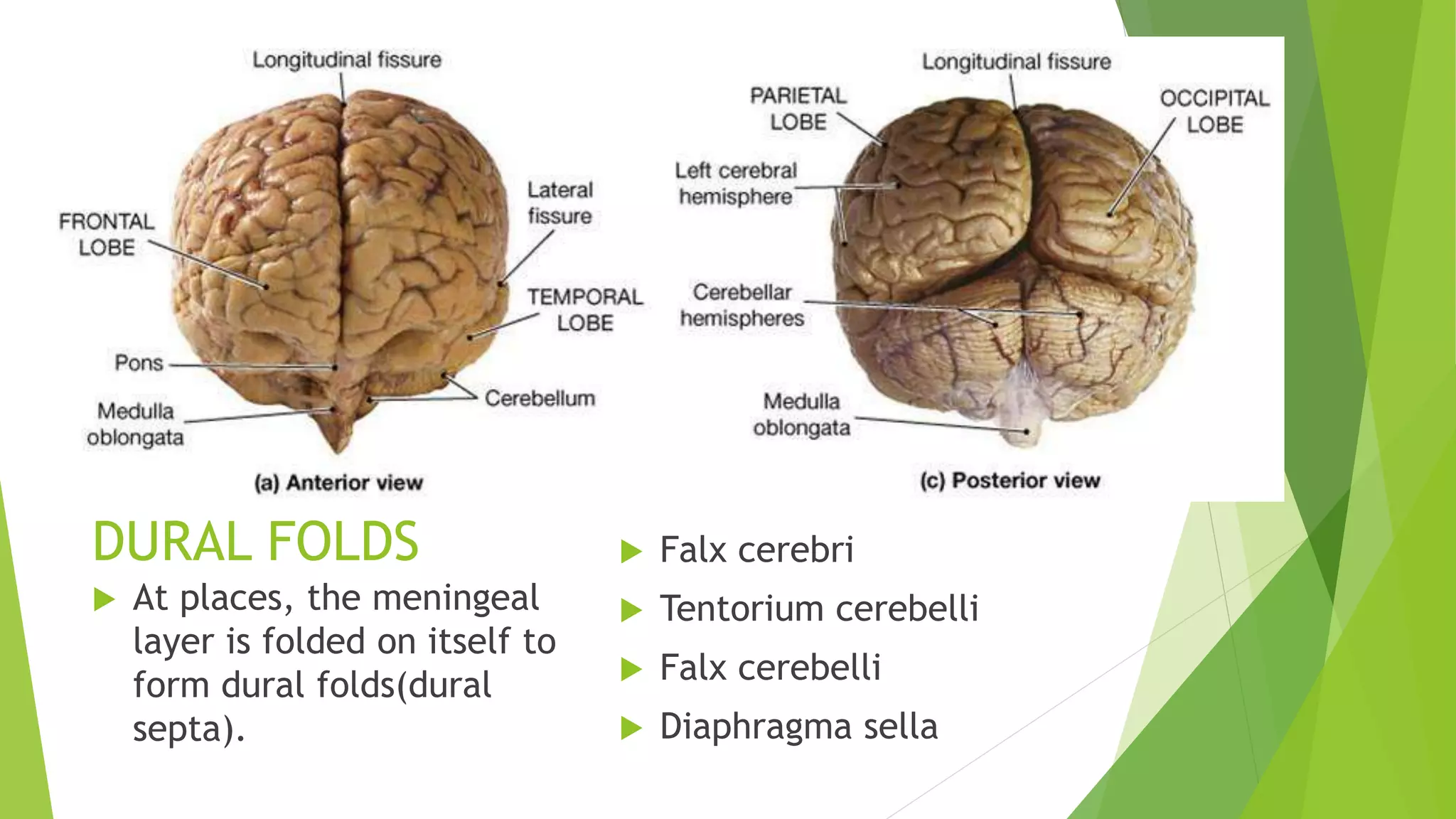
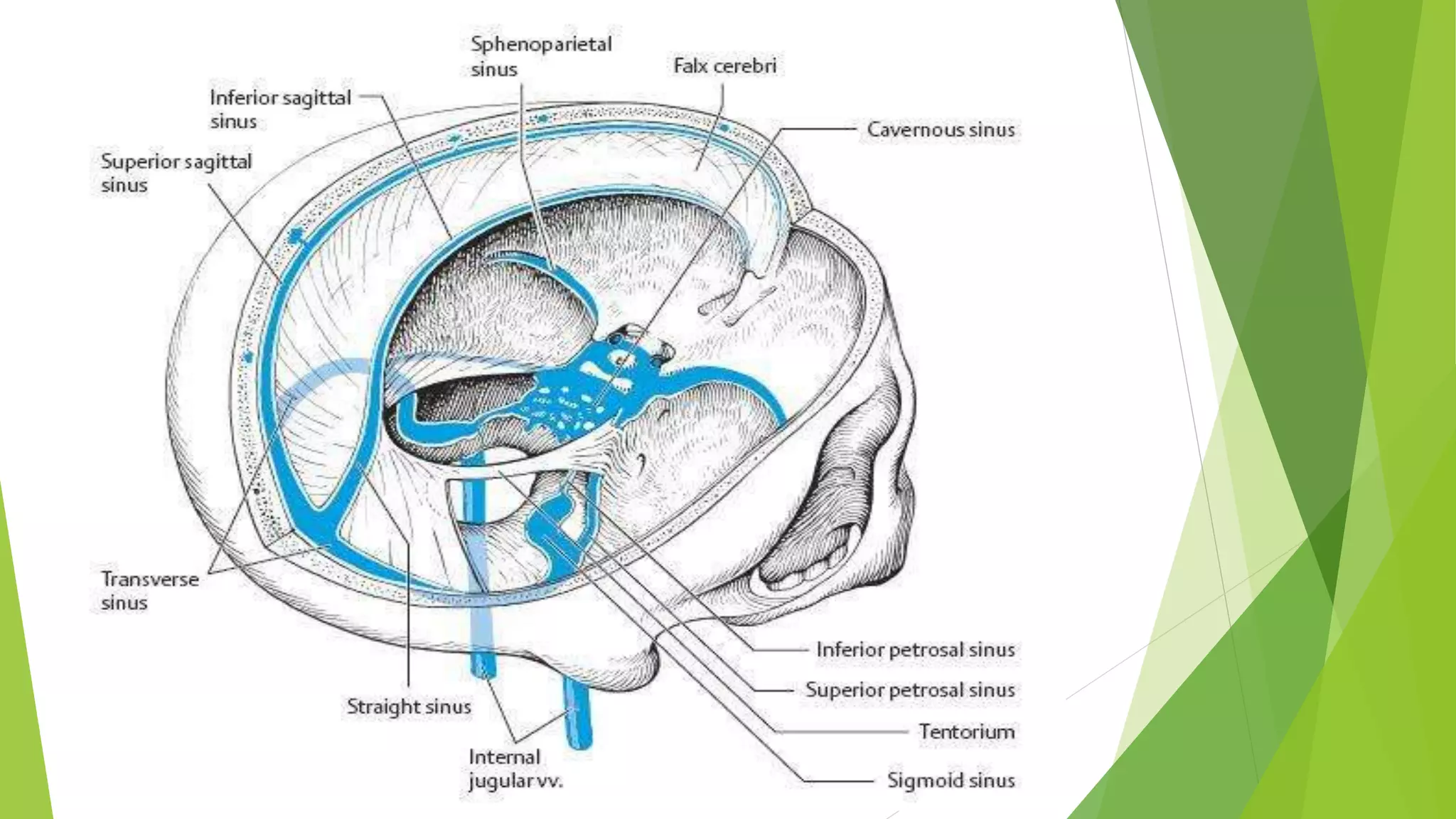
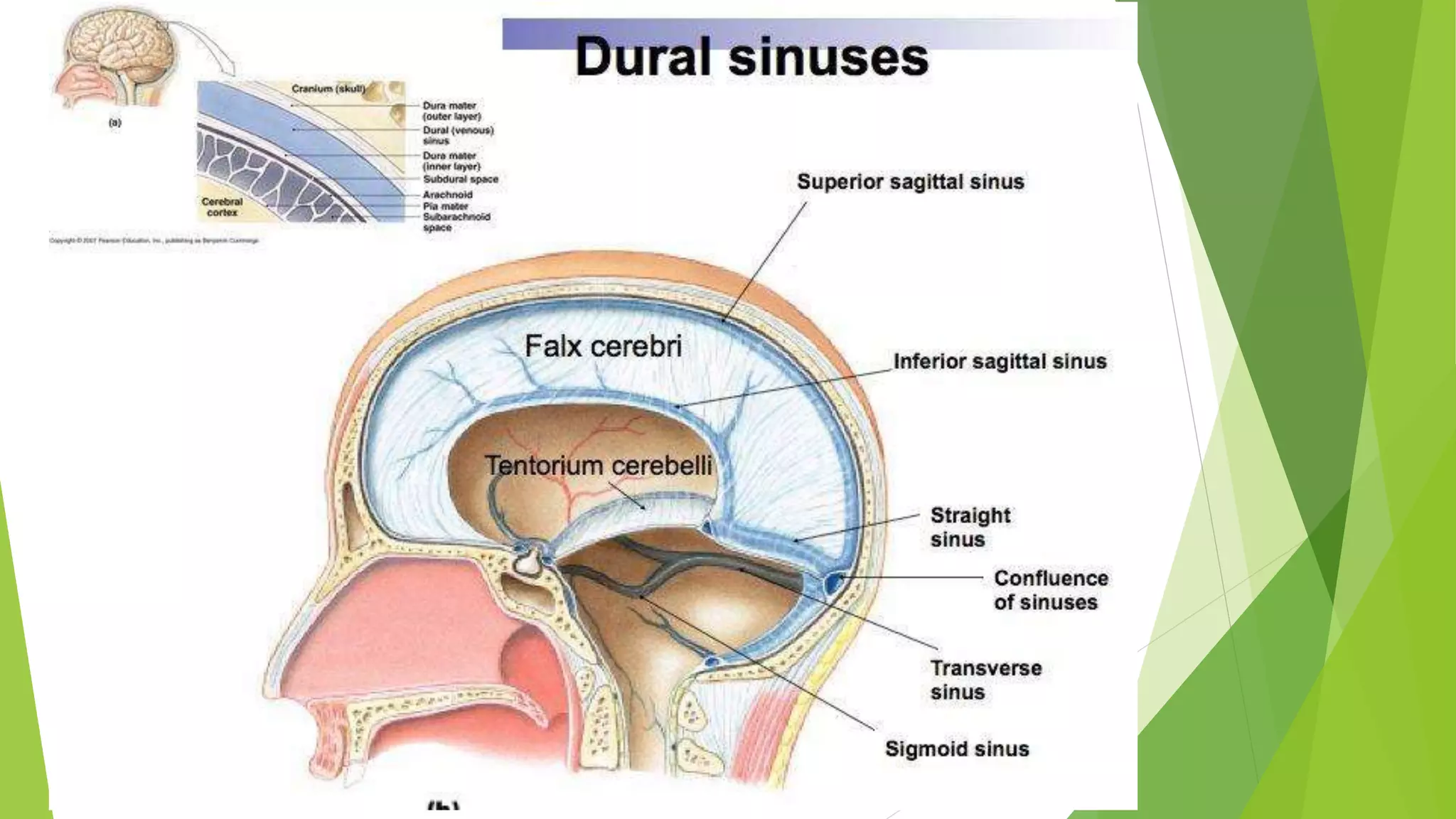
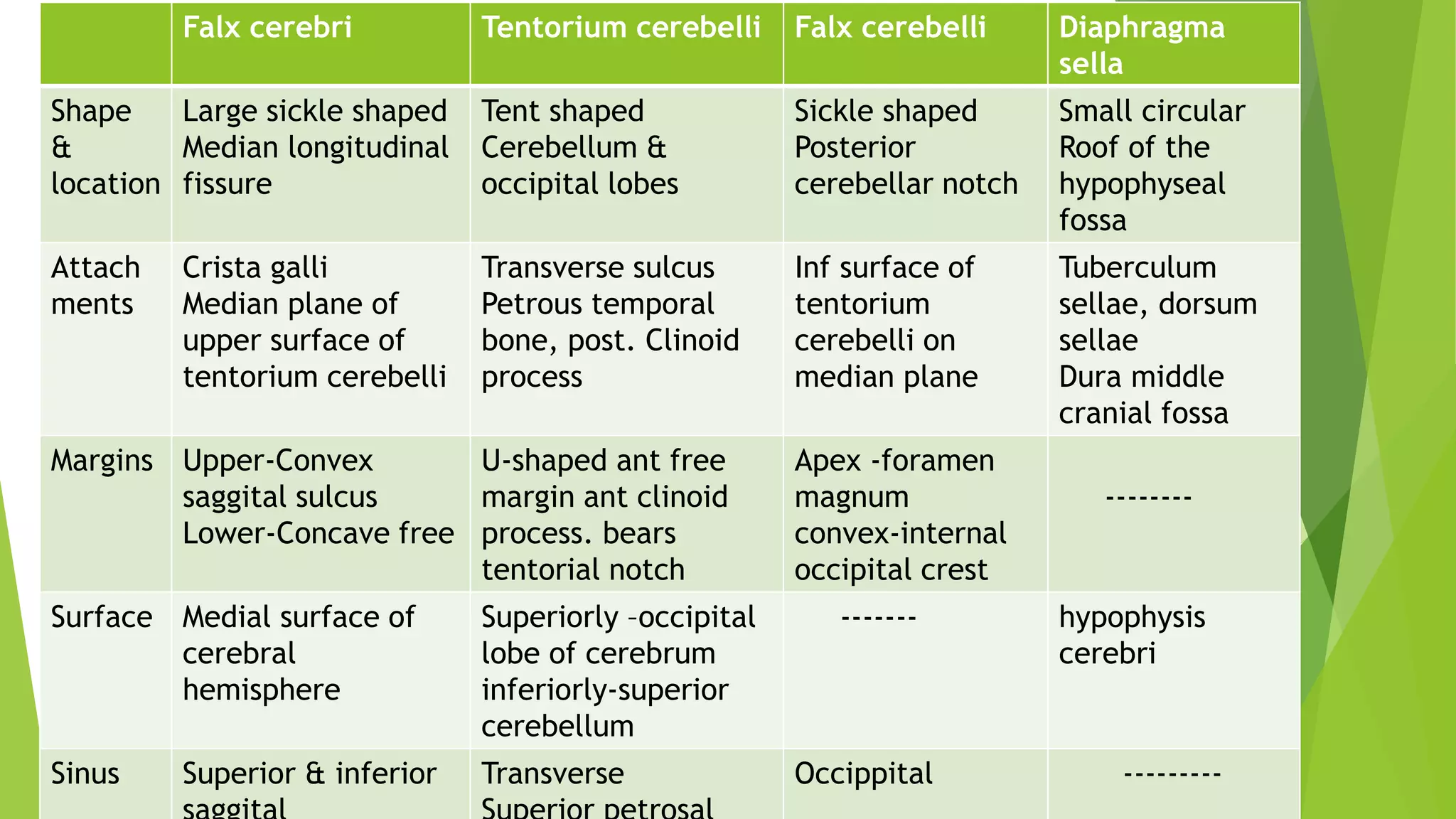

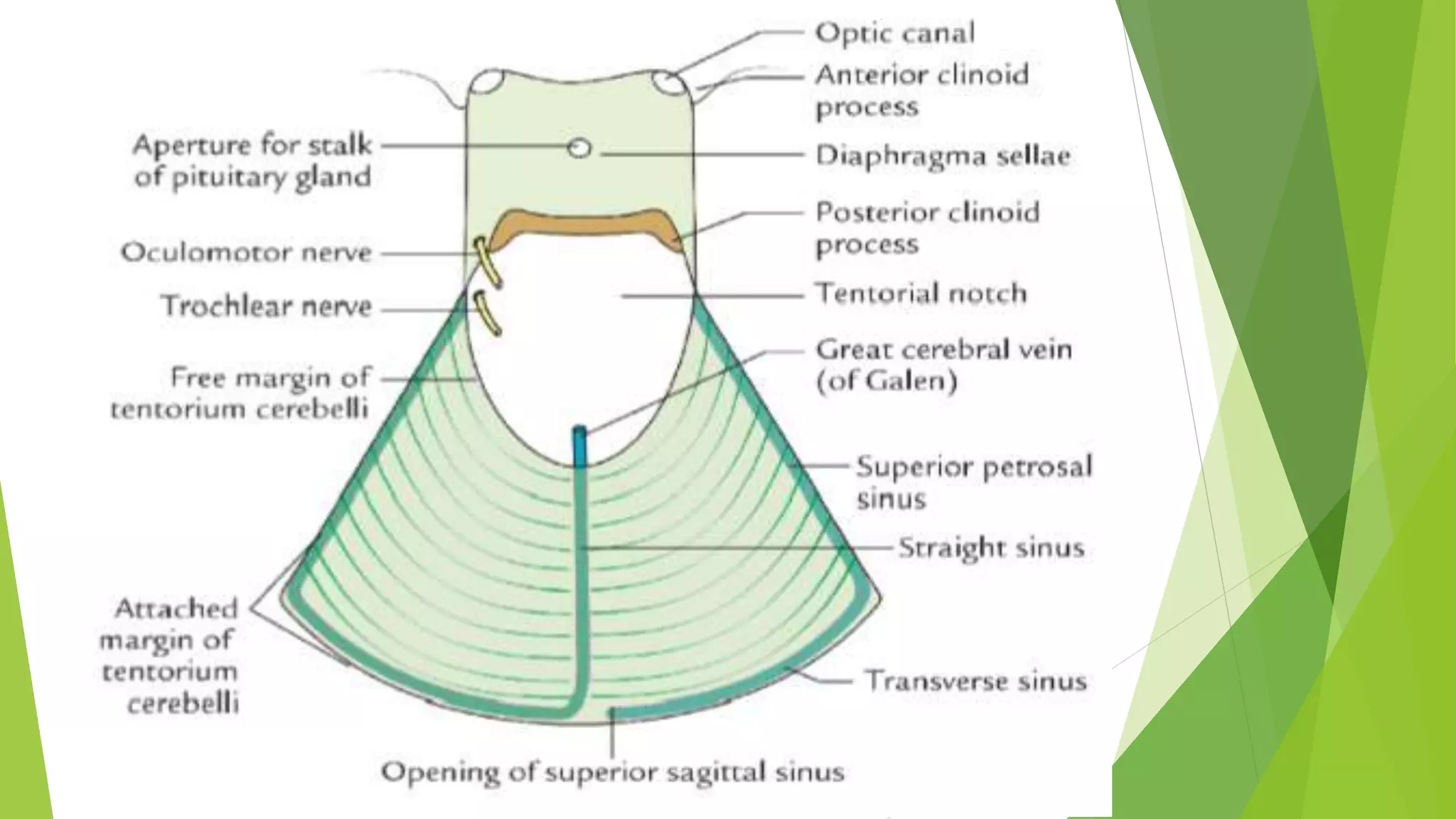
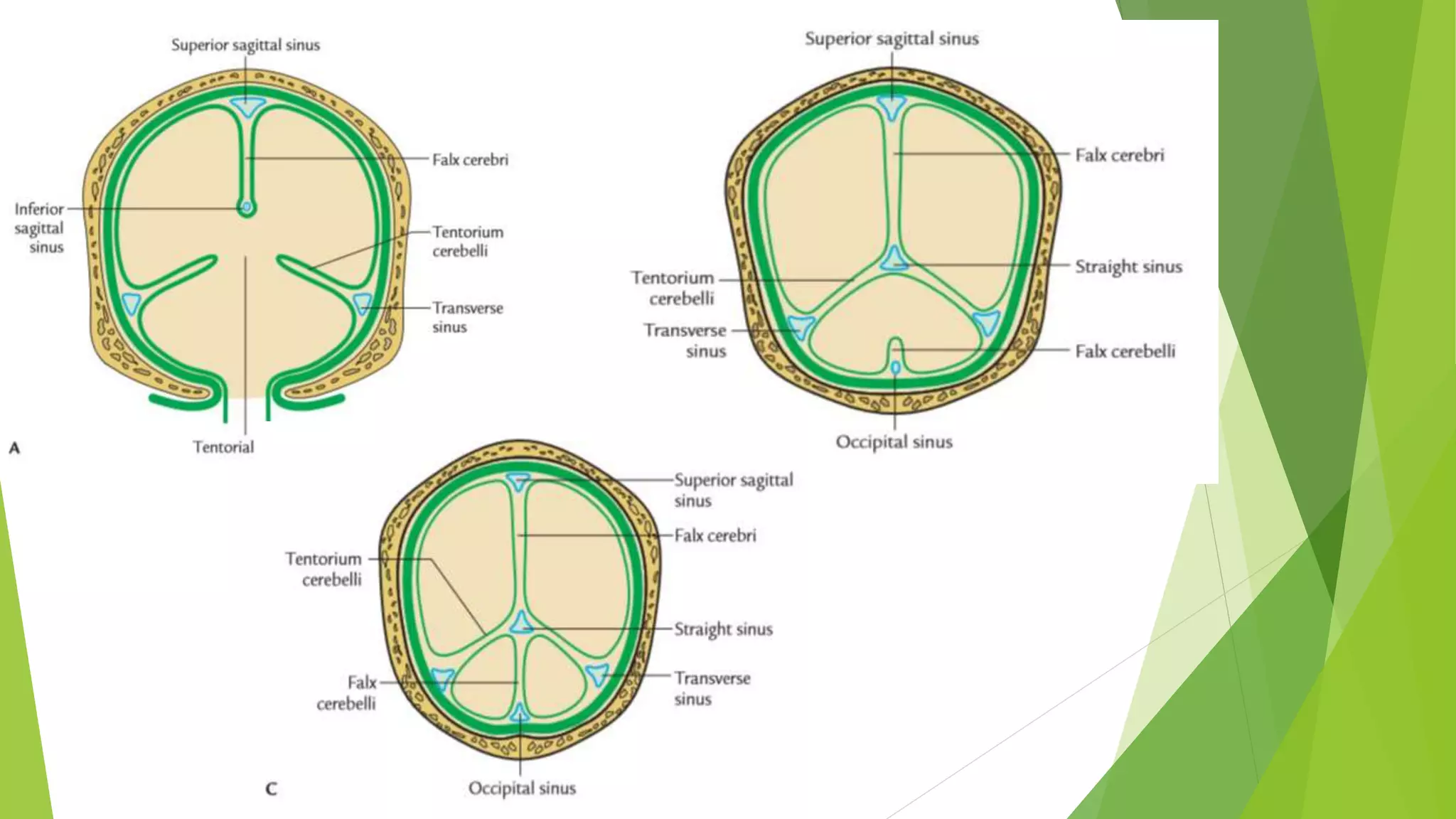

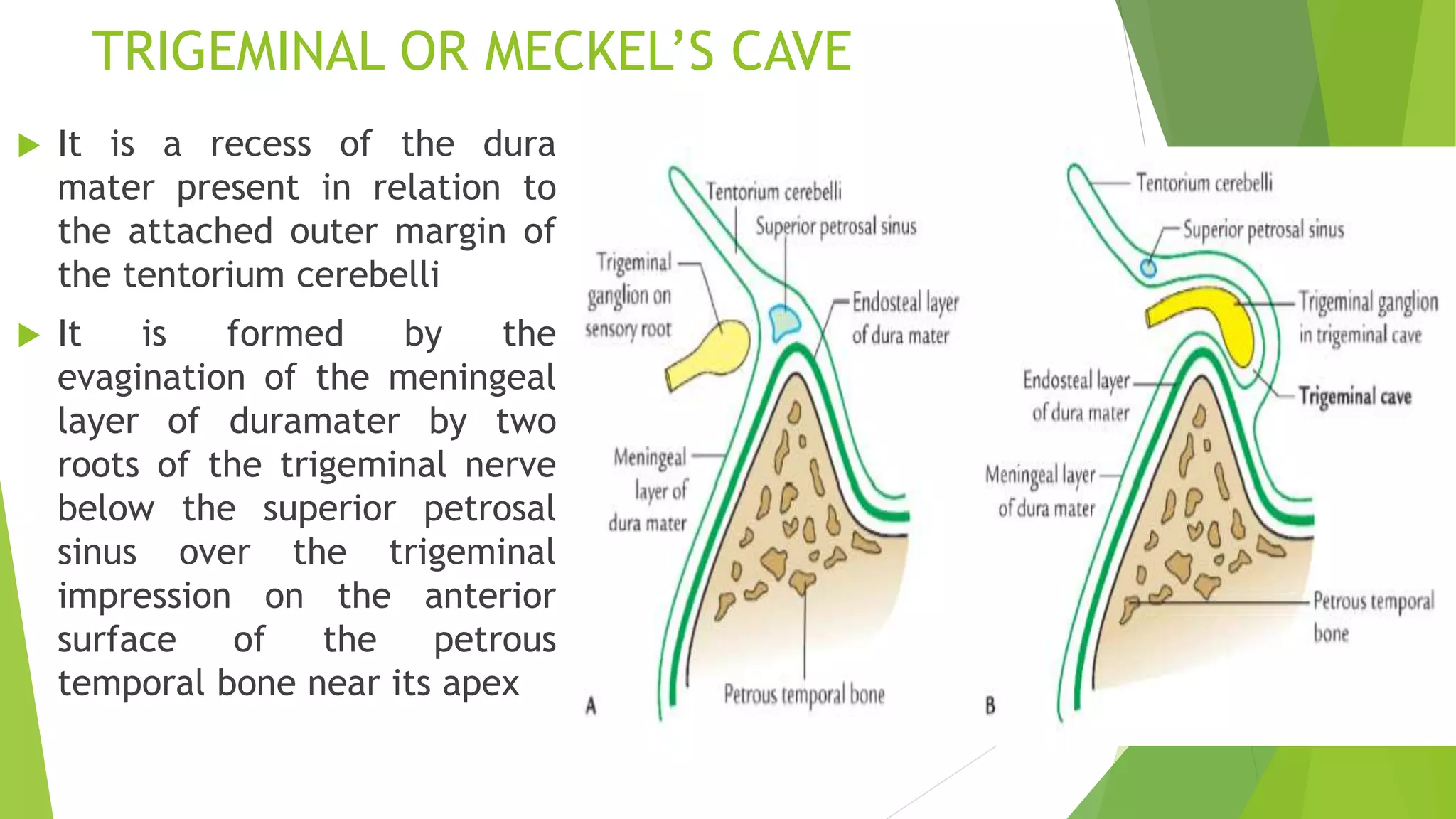


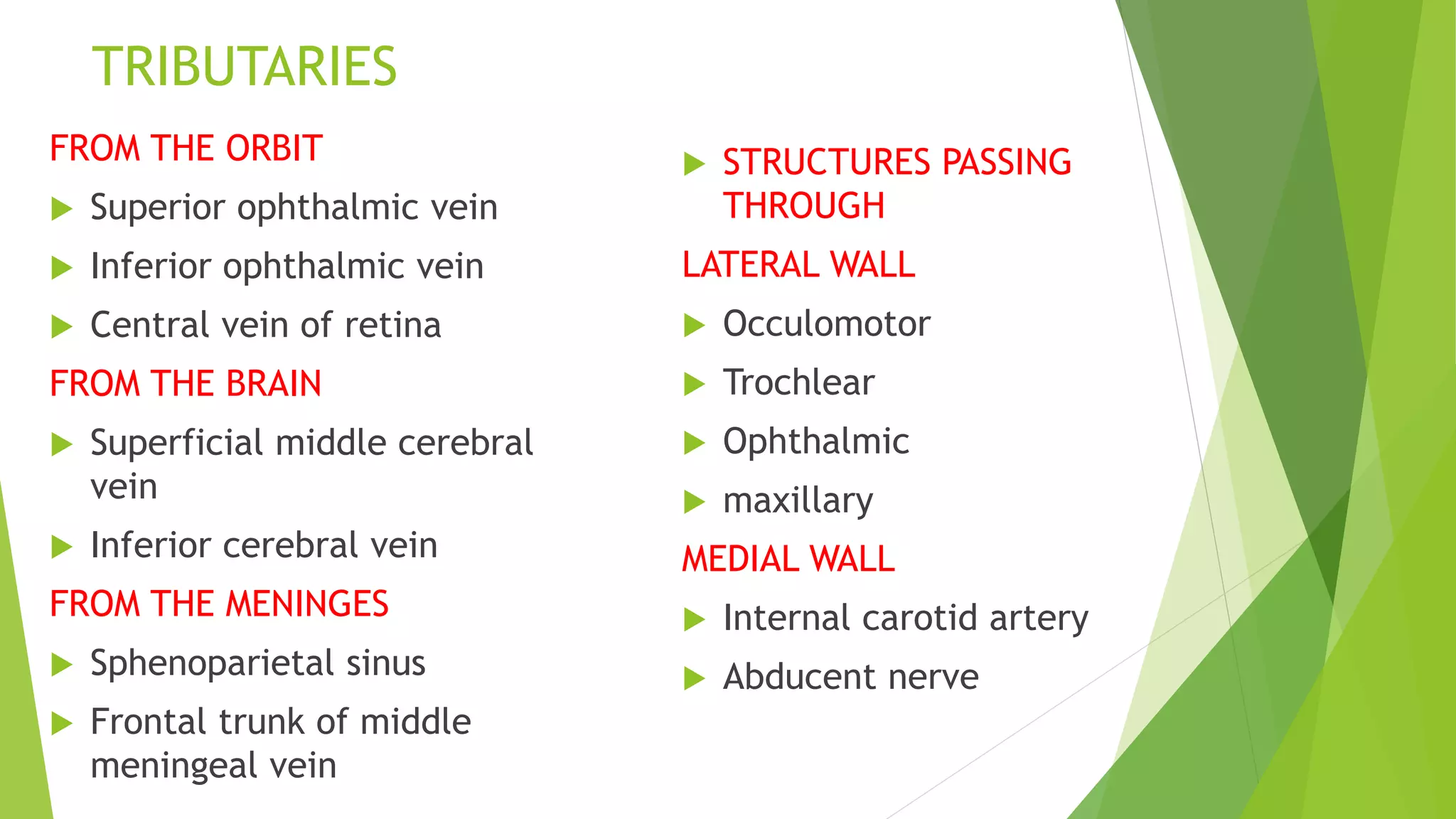
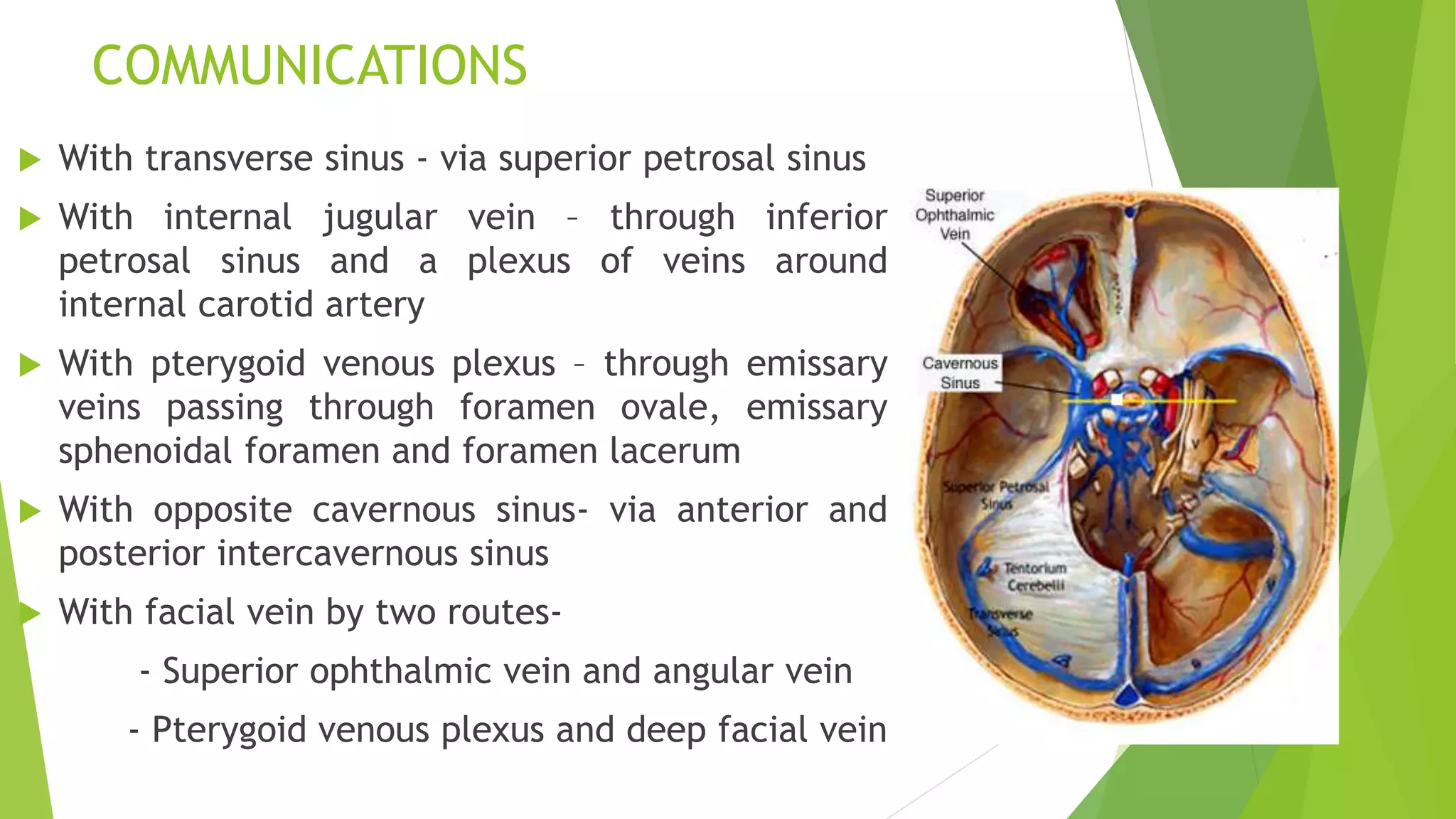


The document summarizes key anatomical structures related to the dura mater and cavernous sinus. It describes the layers of the meninges and identifies four dural folds - the falx cerebri, tentorium cerebelli, falx cerebelli, and diaphragma sella. It also details the location, relations, tributaries, and communications of the cavernous sinus.
























































