Downloaded 17 times




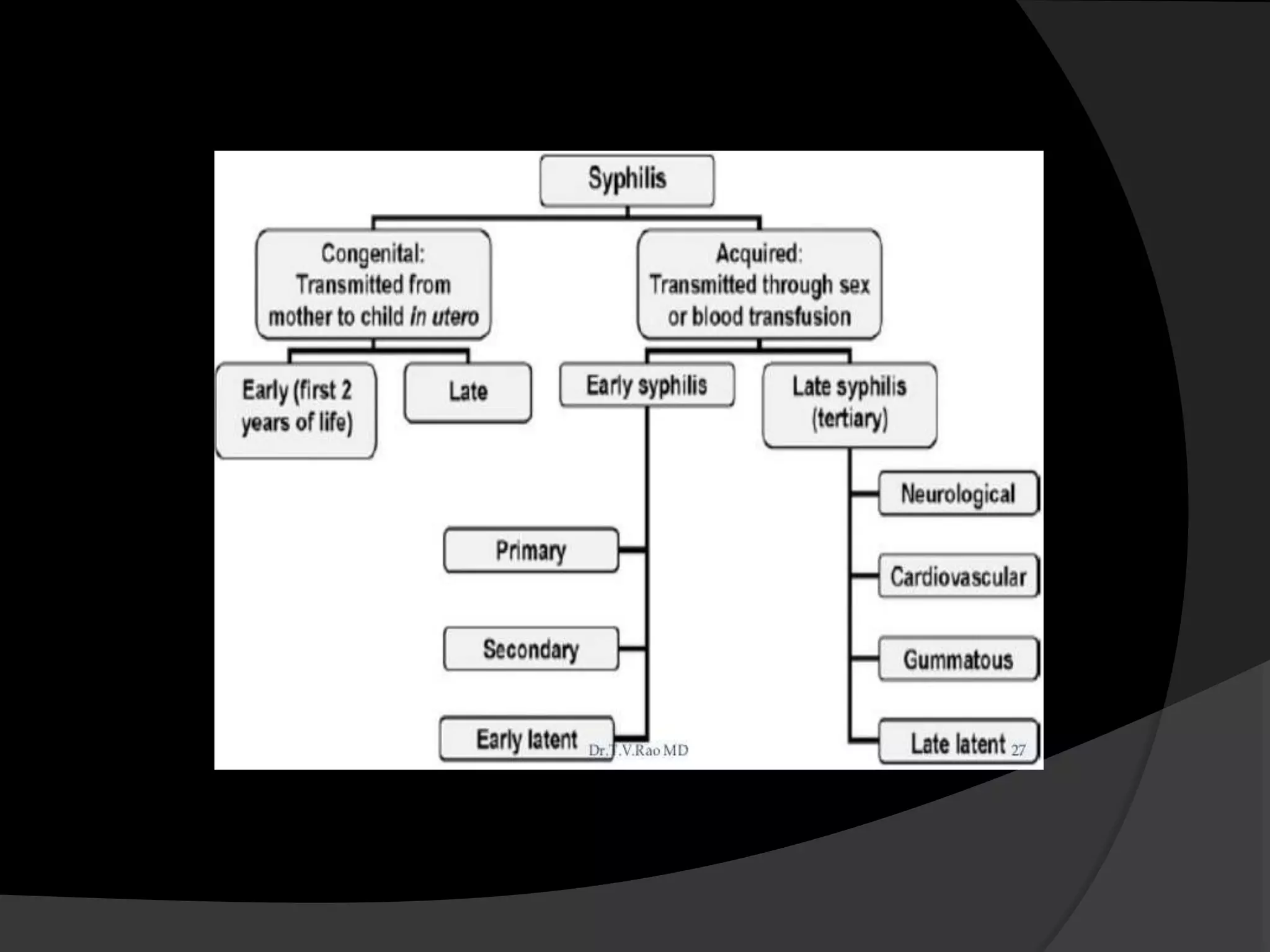





















Syphilis is a sexually transmitted infection caused by Treponema pallidum, characterized by stages: primary (chancre), secondary (rash and lymphadenopathy), latent, and tertiary (organ involvement). Diagnosis involves serological tests, while management typically includes benzathine penicillin. Complications can affect various systems, potentially leading to severe health issues if untreated.



















![1.1.1. bacterial infection of skin [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/1-1-1-bacterialinfectionofskincompatibilitymode-130325014737-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)



































































