Download to read offline




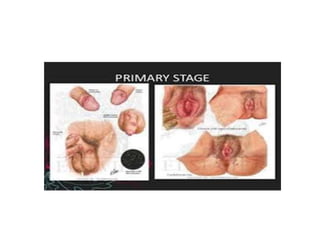


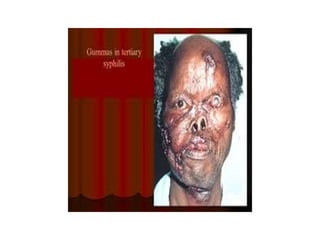



Syphilis is a sexually transmitted infection caused by the bacterium Treponema pallidum. It has four stages - primary, secondary, latent, and tertiary. It is most commonly spread through sexual activity but can also be transmitted from mother to baby. Diagnosis involves blood tests and microscopy. While treatable with antibiotics, syphilis remains a global health problem.


























































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)








