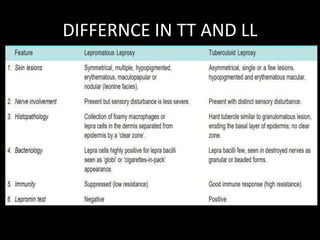
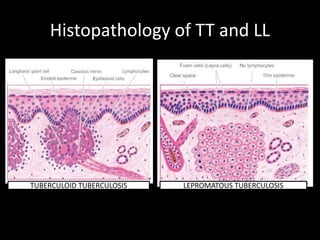
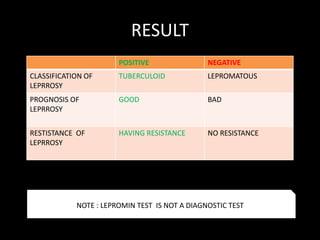
The document presents an overview of leprosy (Hansen's disease), including its causative organism, Mycobacterium leprae, and its various cultivation techniques. It discusses the incidence, modes of transmission, immunology, classifications, diagnostic methods, and treatment protocols such as multi-drug therapy (MDT) for different forms of leprosy. Key points include the lepromin test for classification, the importance of T-cell immune response, and the geographical prevalence of the disease.