Downloaded 274 times

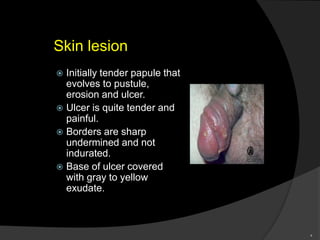





Chancroid is an acute sexually transmitted disease characterized by a painful genital ulcer and painful lymph node swelling. It is caused by the bacteria Haemophilus ducreyi. Incubation is typically 4 to 7 days. Symptoms include tender genital ulcers with well-defined borders and a gray or yellow discharge. Untreated, ulcers can enlarge and buboes may form abscesses. Diagnosis is by gram stain or culture of the ulcer. Treatment is with antibiotics like azithromycin or ceftriaxone. Left untreated, complications can include large draining ulcers or abscesses.





































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
















