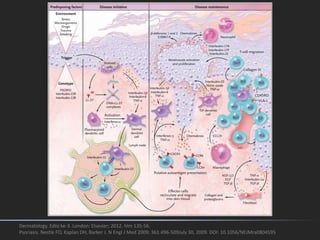
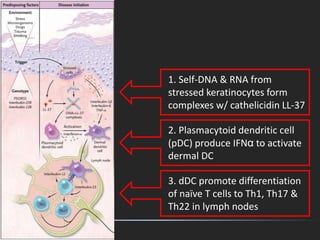
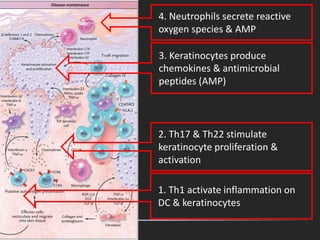
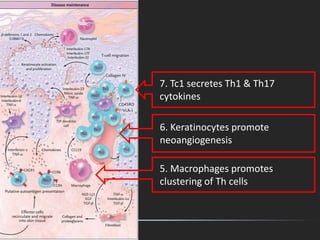













This document discusses papulosquamous disorders, which are characterized by scaly, erythematous papules and plaques. It begins by defining papulosquamous disorders and providing a morphological classification. It then discusses specific disorders like psoriasis, parapsoriasis, and pityriasis rosea. For each disorder, it describes clinical features, pathogenesis, histopathology, and management approaches. The document aims to comprehensively cover papulosquamous disorders through classification, descriptions of individual disorders, and inclusion of relevant images and diagrams.























































































