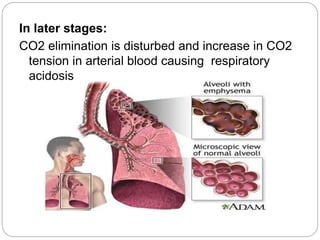
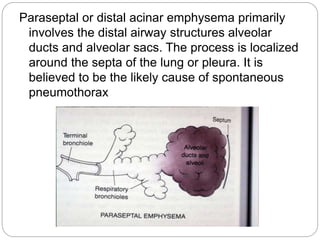
Chronic obstructive pulmonary disease (COPD) refers to two lung diseases, chronic bronchitis and emphysema, that are typically caused by smoking. In COPD, airflow to the lungs is limited by inflammation and damage to airways and lung tissue. Symptoms include cough, sputum production, wheezing, shortness of breath, and weight loss. Treatment focuses on smoking cessation, bronchodilators, oxygen therapy, and managing exacerbations. Nursing care aims to improve ventilation and gas exchange, manage anxiety, and ensure effective airway clearance and rest.