Downloaded 98 times













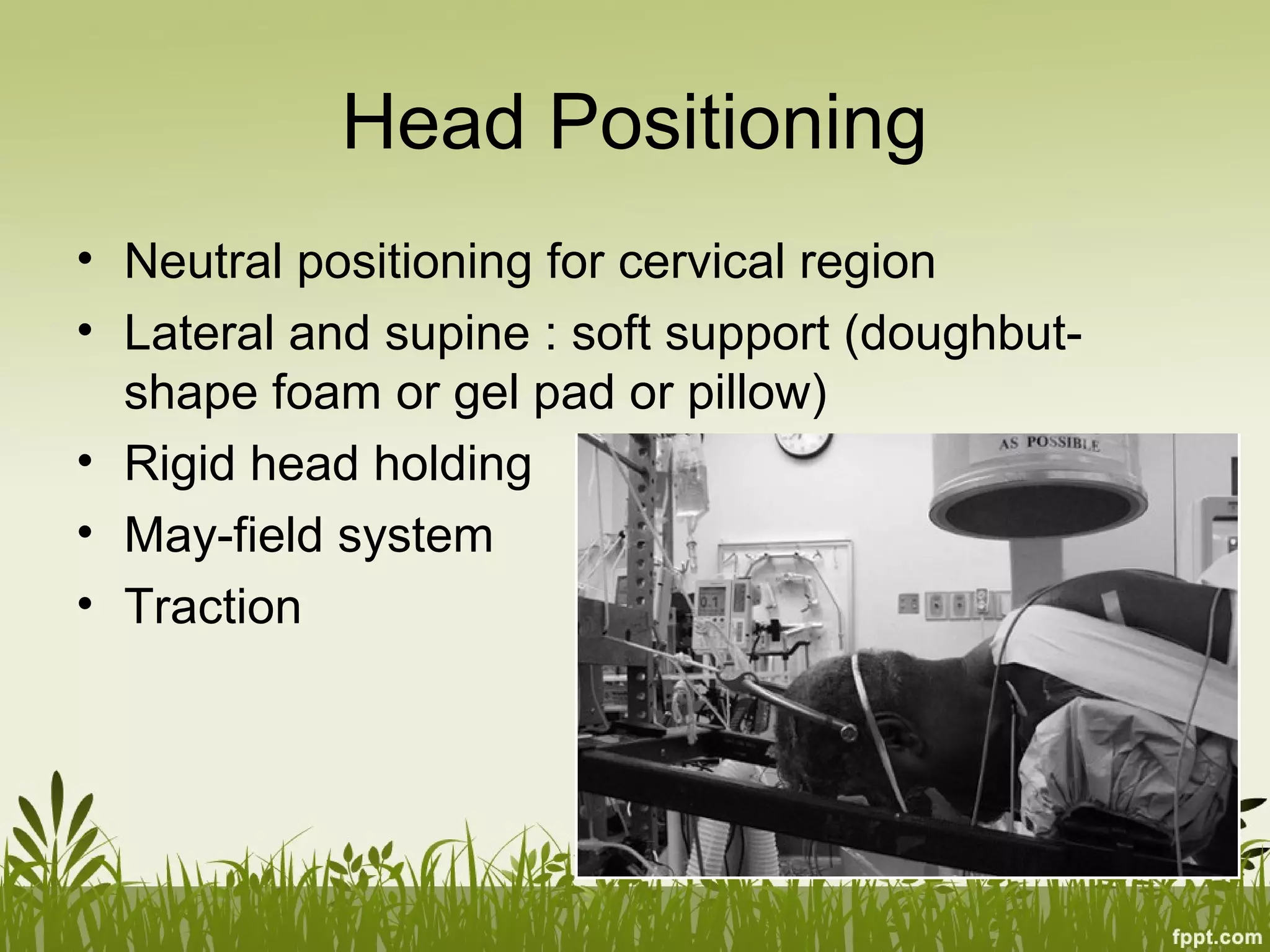









This document discusses patient positioning for various spinal surgeries. It covers the equipment used including tables and head holders. The principles of positioning focus on surgical access, patient safety, spinal alignment, and surgeon ergonomics. Specific risks like neuropathies are reviewed along with how to position for different procedures such as anterior cervical, posterior thoracolumbar fusion, and lateral lumbar approaches. Intraoperative repositioning from prone to supine is also addressed.











































































































