Downloaded 158 times

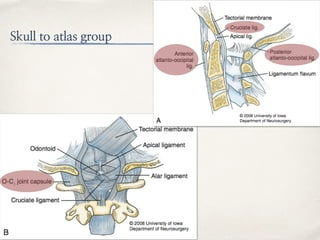

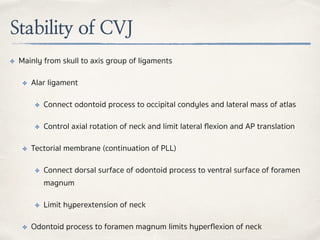
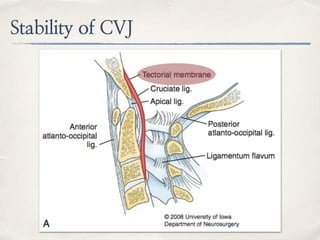
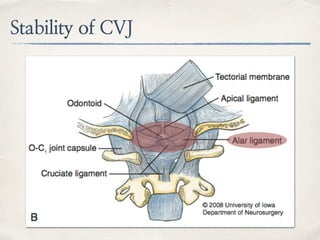
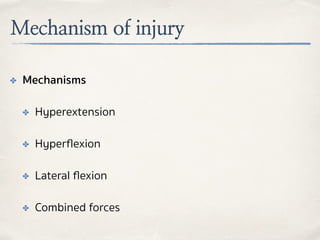
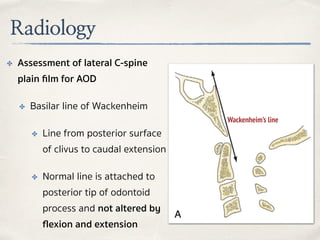
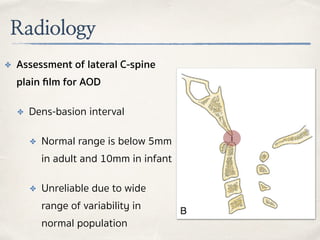
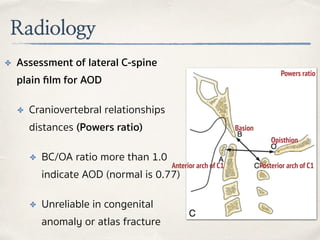
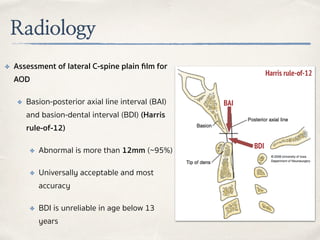

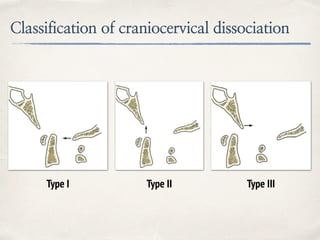


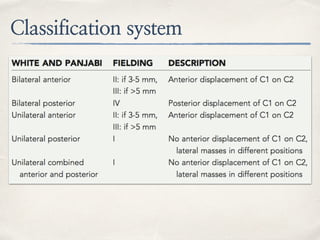


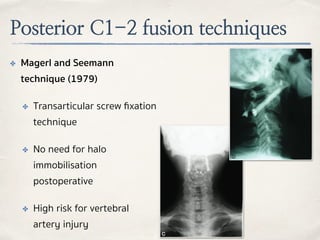
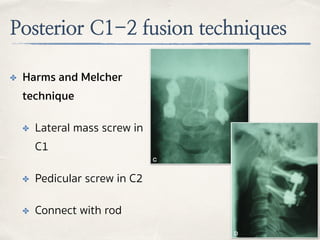



This document discusses evaluation and management of craniocervical dissociation and atlantoaxial injuries. It covers anatomy of the craniocervical junction, mechanisms of injury, classification systems, diagnosis using imaging, and treatment considerations including traction, fusion techniques. Key points are stability from skull to axis ligaments, most common injury is hyperextension with lateral flexion, and treatment depends on injury type and may involve traction or anterior-posterior fusion.










































































































