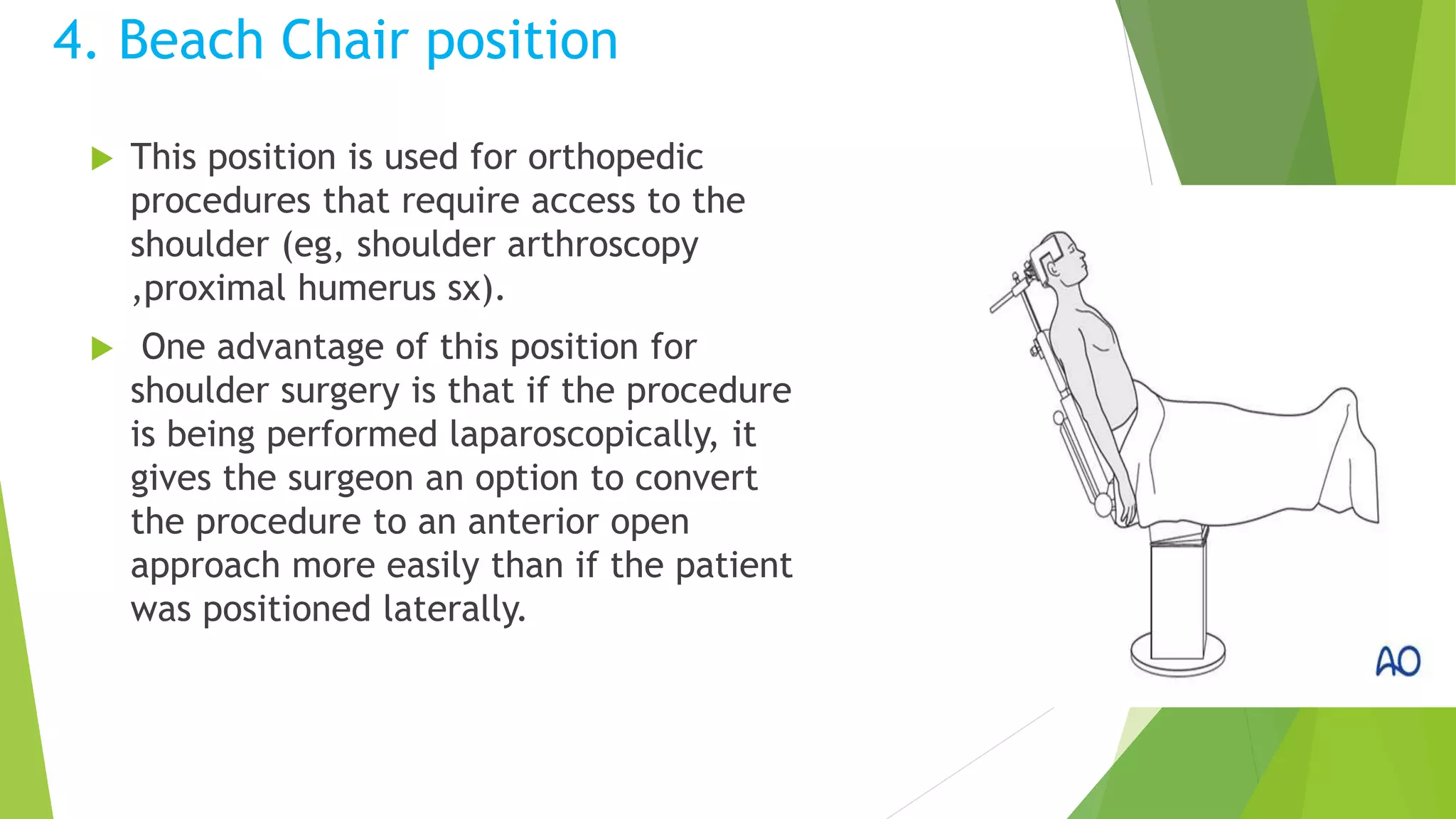
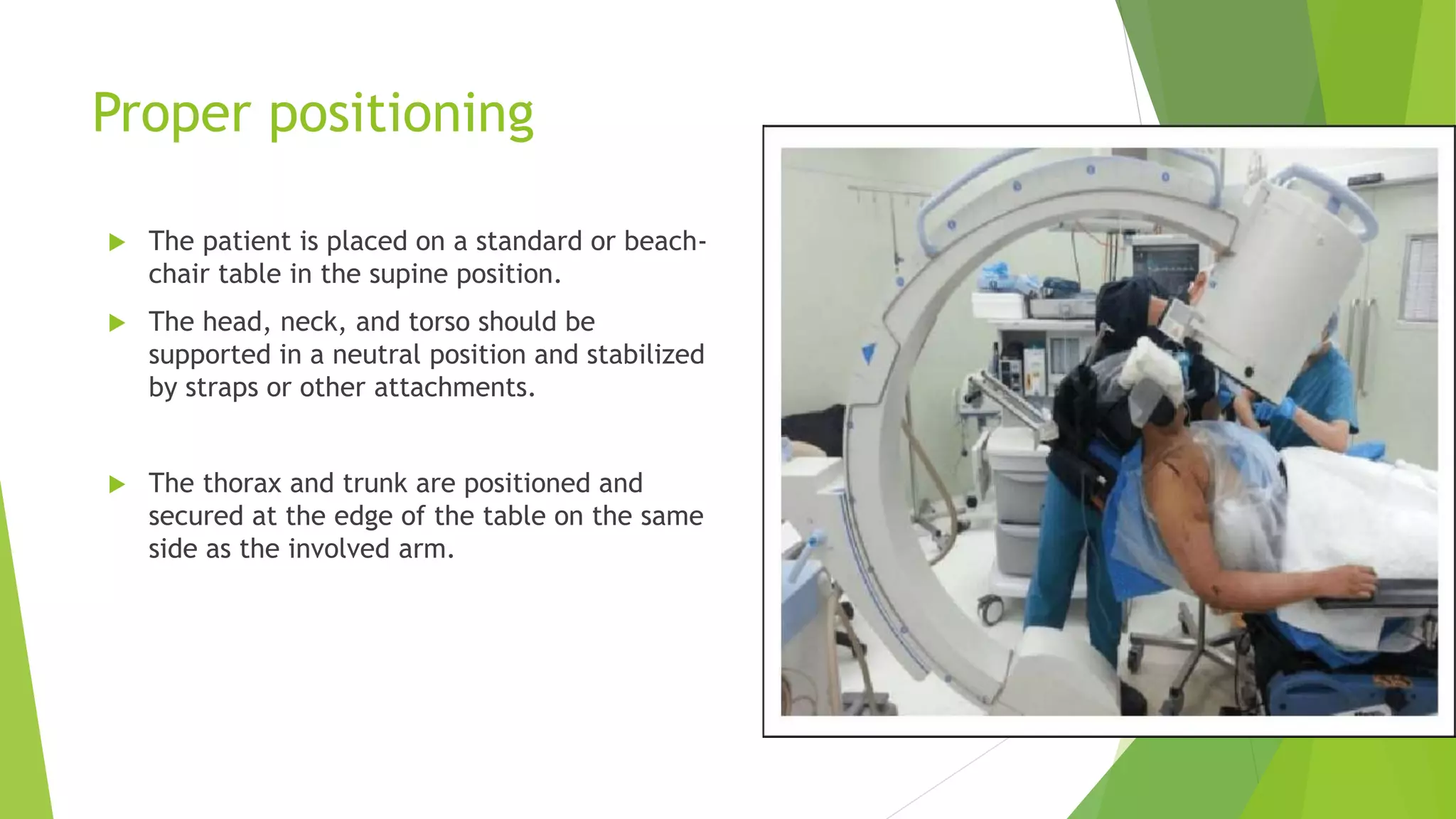
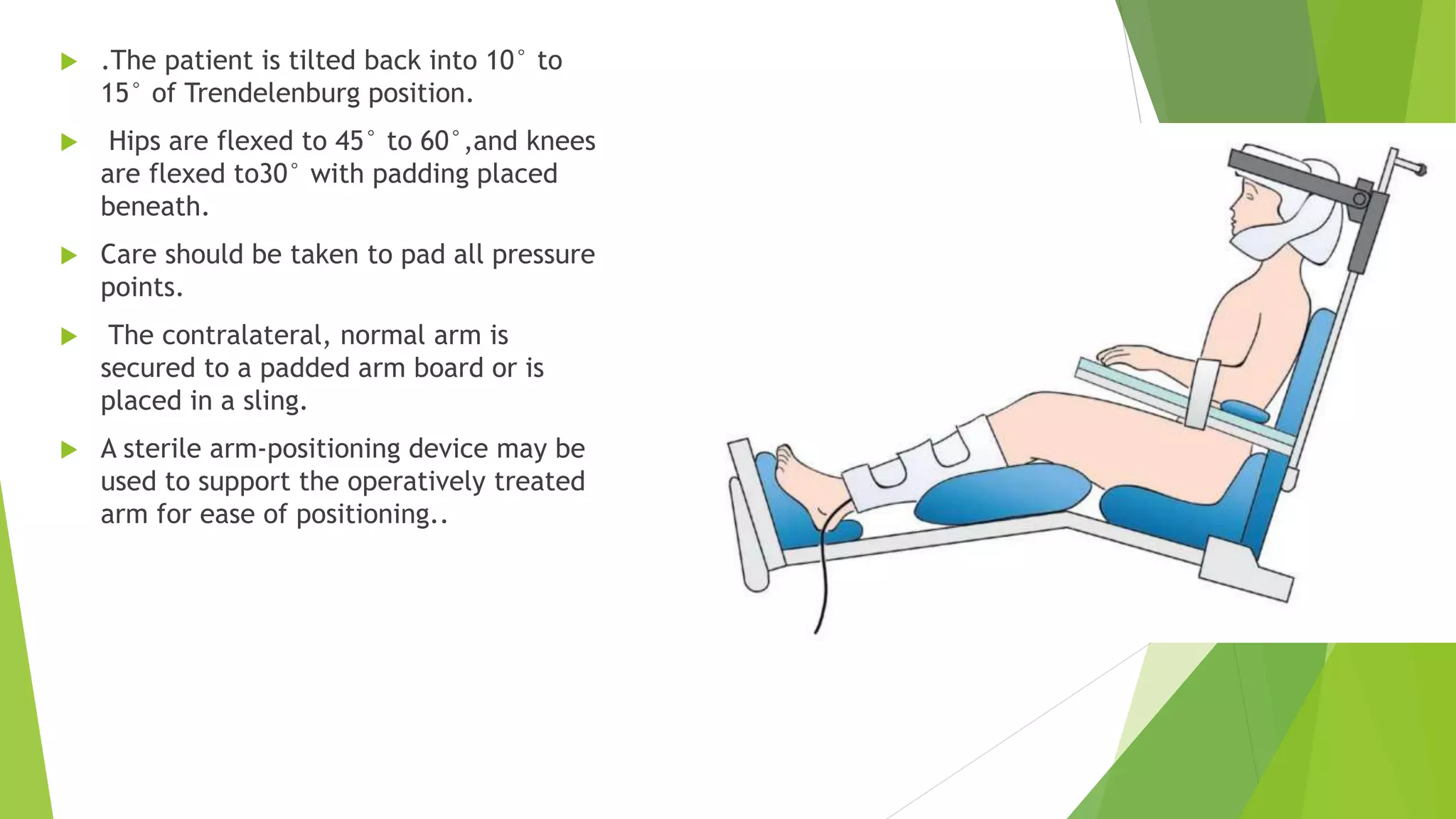
The document emphasizes the significance of proper patient positioning in orthopedic surgeries to minimize complications and ensure safety. It outlines various positions used during surgery, such as supine, prone, lateral, and beach chair positions, detailing the necessary precautions to avoid specific risks associated with each. Additionally, it discusses the challenges faced when positioning elderly, obese, and pediatric patients, along with the importance of ongoing assessment throughout the surgical procedure.