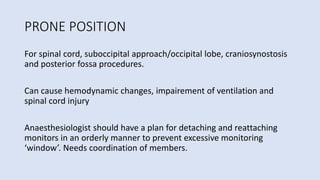
1) Proper positioning is important in neurosurgery to optimize exposure while ensuring patient safety and physiological stability. Different positions like supine, prone, lateral and sitting are used depending on the surgical site.
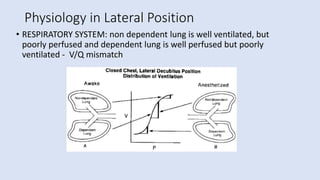
2) Positions can affect respiratory, cardiovascular and central nervous systems through changes in venous return, ventilation/perfusion matching, intracranial pressure and nerve stretching. Careful positioning and monitoring are needed to prevent complications.
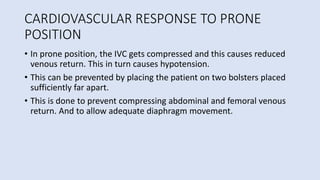
3) Special equipment like Mayfield head holders, horseshoe frames and Wilson frames help achieve and maintain desired positions for optimal surgical access and exposure.






![Prevent injury to Brachial Plexus
• Arms should NOT be abducted >90⁰; elbows shouldnt be
extended>90⁰ [90-90 position]
• Elbow should be anterior to the shoulder to prevent wrapping of
brachial plexus around head of humerus
• Pronation makes ulnar nerve very vulnerable, while supination keeps
it in a more protected position](https://image.slidesharecdn.com/positioninginneuroanaesthesiahimanshubaxy-240221194156-c52d4678/85/DIFFERENT-POSITIONING-IN-NEUROANAESTHESIA-23-320.jpg)
![SITTING POSITION
• Modified recumbent position
• Skull secured in three pin head holder
[applied while on supine].
• Infiltration of scalp & periosteum @ pin
sites
• Legs placed in thigh-high compression
stockings](https://image.slidesharecdn.com/positioninginneuroanaesthesiahimanshubaxy-240221194156-c52d4678/85/DIFFERENT-POSITIONING-IN-NEUROANAESTHESIA-30-320.jpg)
![EQUIPMENTS USED FOR POSTIONING IN
NEUROSURGERIES
1) Pin (Mayfield) head holder
• Skull block before application
• Placed in a band like area just above orbits & pinna [~sweatband]
• Avoid over thin temporal bone; caution when over frontal sinus
• Coated with antibiotic ointment](https://image.slidesharecdn.com/positioninginneuroanaesthesiahimanshubaxy-240221194156-c52d4678/85/DIFFERENT-POSITIONING-IN-NEUROANAESTHESIA-35-320.jpg)