Downloaded 121 times






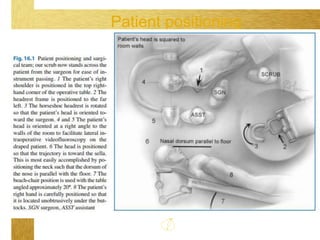

























This document provides information about transsphenoidal approaches for pituitary surgery. It discusses the surgical technique including patient positioning, the nasal phase involving sublabial or endonasal incisions, the sphenoid phase to access the sella turcica, the sellar phase of tumor resection, and reconstruction/closure. Complications are also outlined such as hypothalamic injury, visual damage, vascular issues, cerebrospinal fluid leaks, and nasal/sinus problems. The document provides a detailed overview of the surgical procedure and risks involved in transsphenoidal pituitary surgery.











































































































