Downloaded 16 times
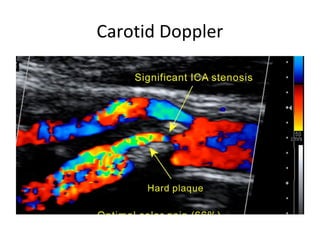
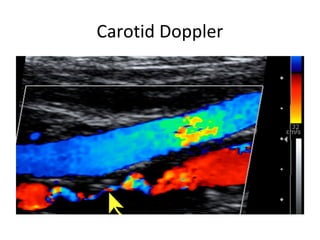
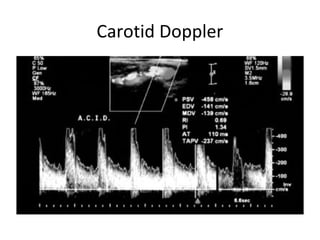
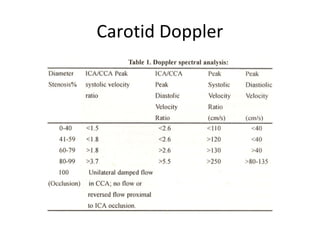
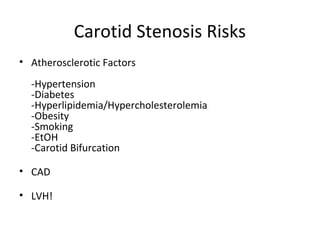
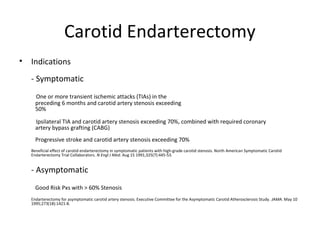
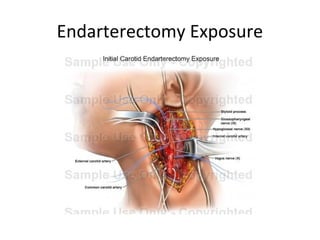

A 77-year-old female presented to the emergency department with difficulty breathing and was found to have pulmonary edema and left ventricular hypertrophy. During her hospital stay, a carotid bruit was discovered and Doppler ultrasound revealed 80-99% stenosis of the right carotid artery. She was scheduled for a right carotid endarterectomy to address the high-grade stenosis, a procedure she tolerated well without complications. Medical management has improved for asymptomatic carotid stenosis but intervention may still benefit high-risk patients.































































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)











