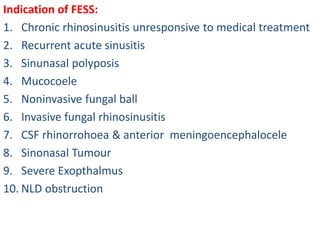
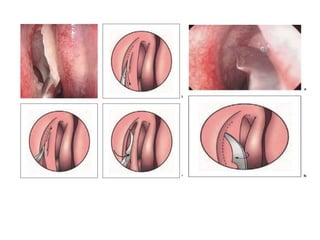
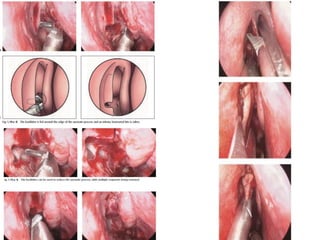
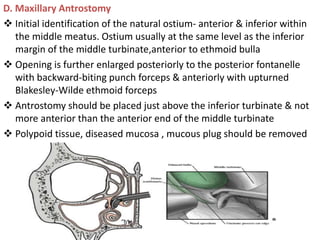
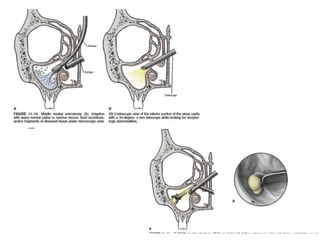
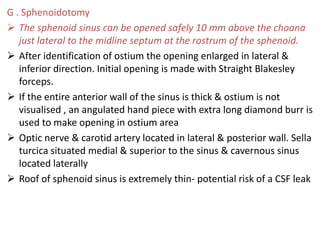
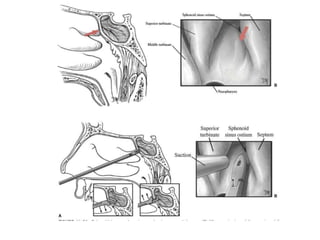
The document discusses Functional Endoscopic Sinus Surgery (FESS). FESS is a minimally invasive procedure that uses an endoscope to access and treat the paranasal sinuses. It aims to restore sinus function by re-establishing ventilation and mucociliary clearance. Key steps in FESS include uncinectomy to remove the uncinate process, maxillary antrostomy to access the maxillary sinus, and ethmoidectomy to access the ethmoid sinuses. Proper identification of anatomical landmarks like the middle turbinate, uncinate process, and bulla ethmoidalis is important for successful FESS.