Downloaded 319 times
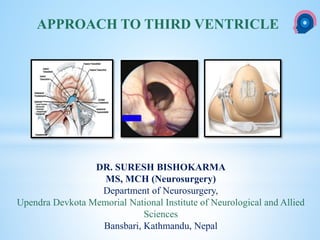
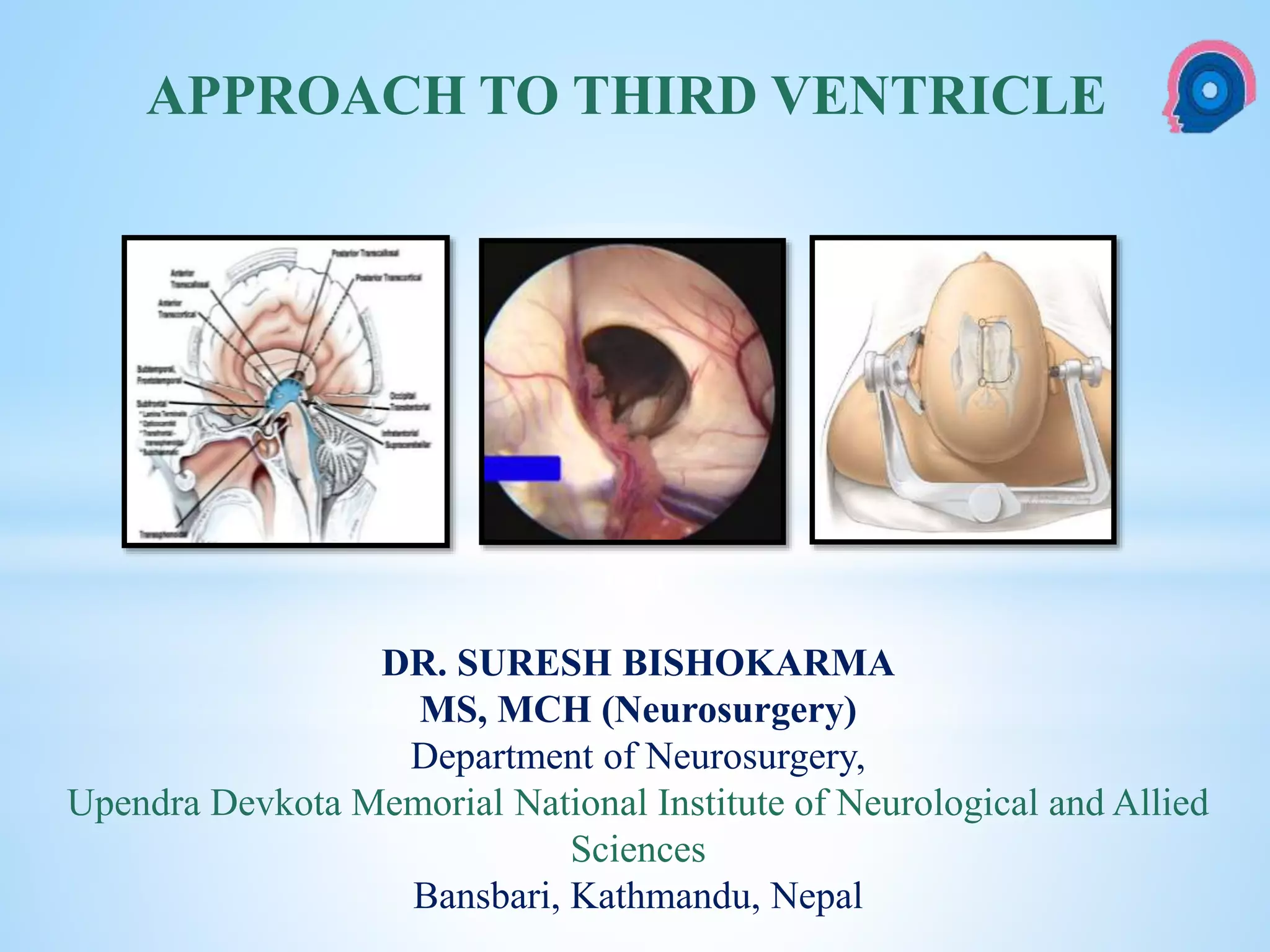
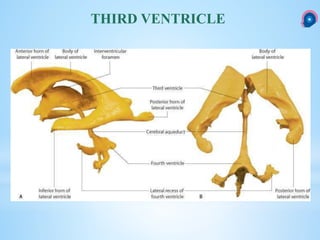
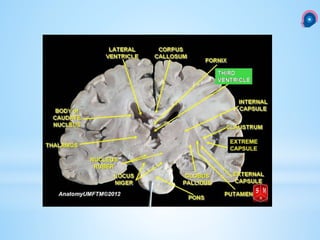
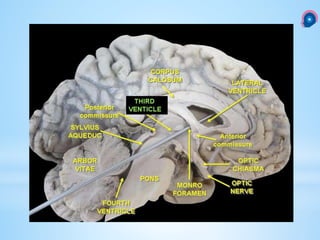
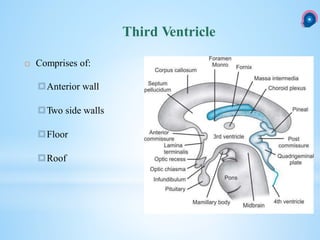
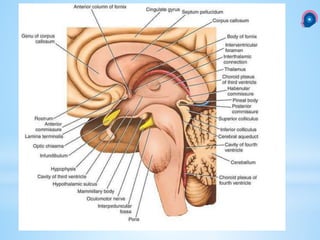
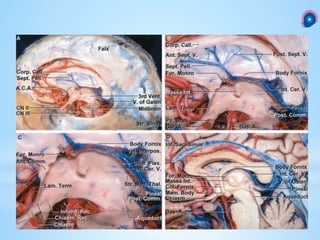
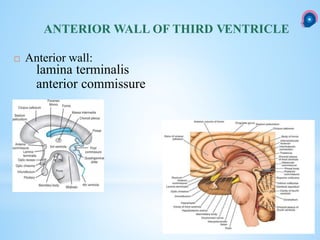
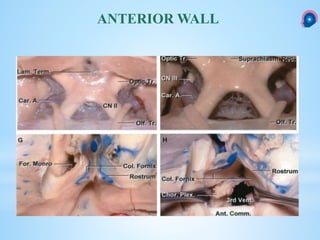
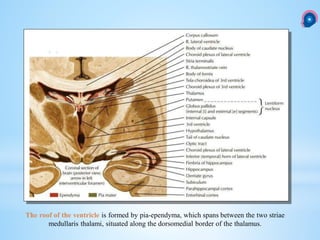
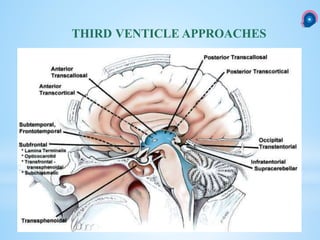
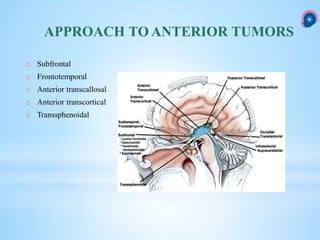

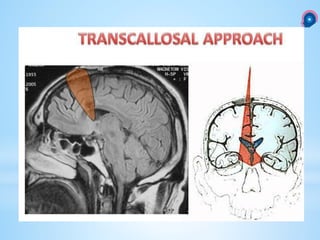
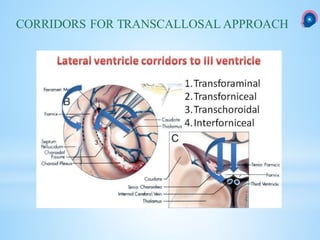
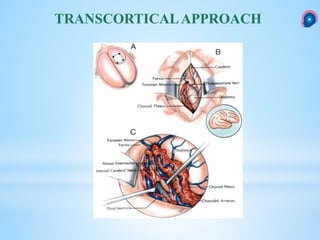
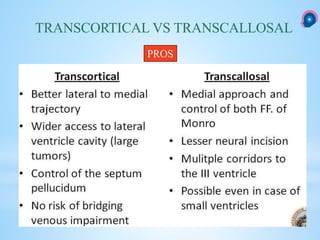
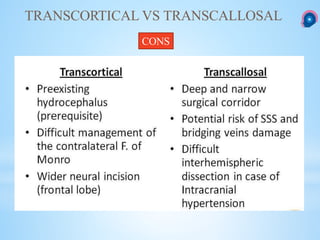
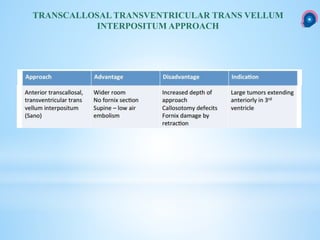
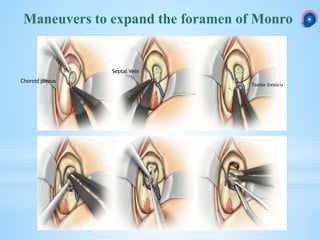
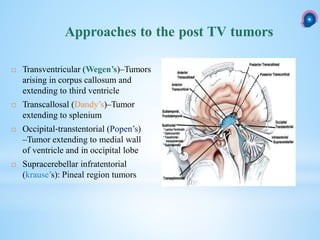
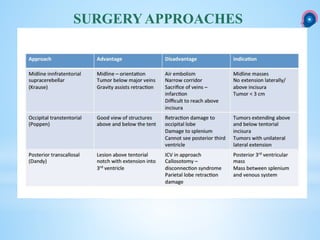
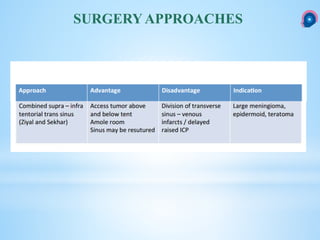
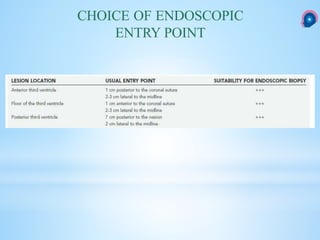
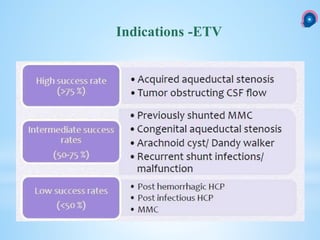
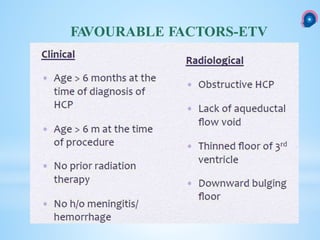
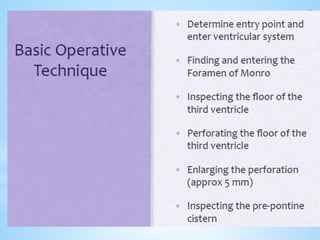
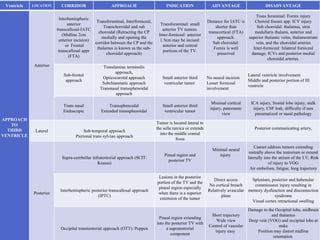

The document discusses the history, anatomy, and surgical approaches related to the third ventricle of the brain. It outlines various techniques for accessing and treating tumors within the third ventricle, including the endoscopic third ventriculostomy and various microsurgical techniques. Additionally, it highlights complications and considerations for different surgical corridors when approaching the third ventricle.








































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)














