Downloaded 121 times


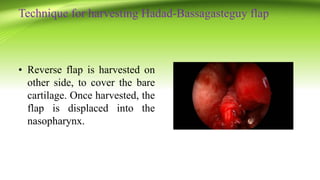
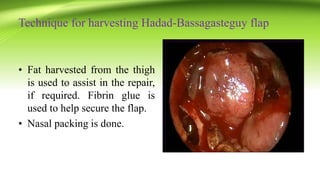
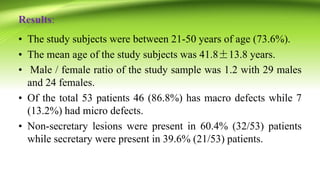
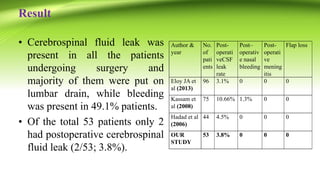

The document discusses the use of the Hadad-Bassagasteguy (HB) flap in reconstructing anterior skull base defects after endonasal skull base surgery. The HB flap uses the vascularized nasal septal mucoperiosteum to repair defects. In a study of 53 patients who underwent HB flap reconstruction, only 2 patients (3.8%) experienced post-operative cerebrospinal fluid leaks. The study found the HB flap to be effective at preventing post-operative CSF leaks across a variety of patient profiles and skull base surgery types. The HB flap is becoming a standard technique for reconstructing anterior skull base defects due to its high success rate and versatility.











































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)

![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

