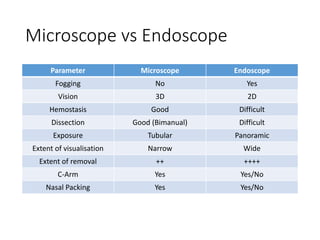
Dr. Rahul Jain presented on endonasal endoscopic anatomy, detailing the evolution of transsphenoidal pituitary surgery and the advantages of using an endoscope over a microscope. Key topics included the anatomical structures involved, variations in sinonasal anatomy, vasculature supply, and stages in endoscopic trans-sphenoidal surgery. The presentation emphasized the importance of identifying landmarks for safe surgical exposure and techniques for effective reconstruction post-surgery.