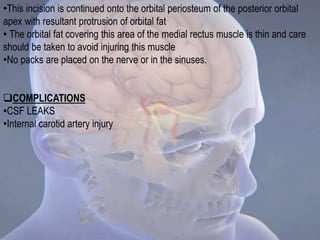
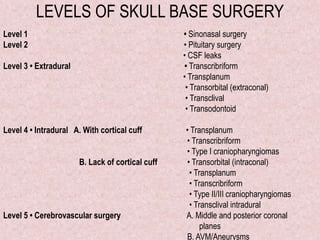
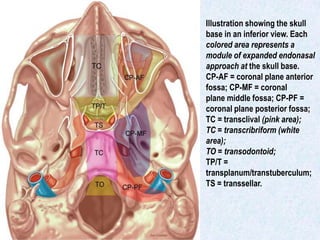
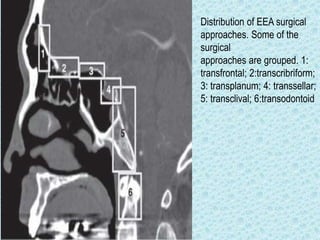
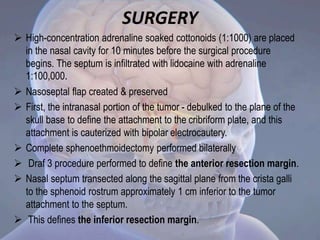
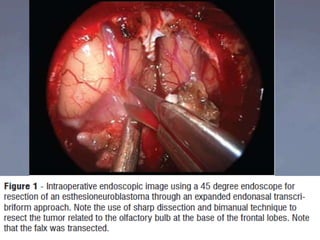
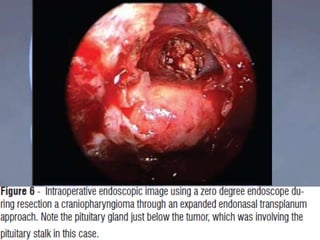
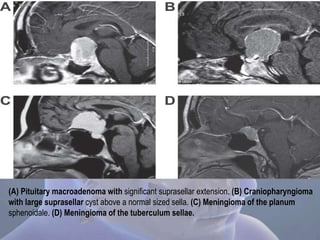
This document discusses different levels and approaches for endoscopic skull base surgery. It focuses on the transcribriform and transplanum approaches. The transcribriform approach involves removing the cribriform plate to access the anterior skull base. It is used for anterior skull base meningiomas and esthesioneuroblastomas. The transplanum approach removes the planum sphenoidale and tuberculum sellae to reach lesions in the suprasellar region, such as pituitary adenomas and craniopharyngiomas. Both approaches aim to devascularize the tumor early and resect attachments to the skull base. Care must be taken to avoid critical neurovascular structures during resection.

![DIAGNOSTIC WORK UP
• Physical examination-neurologic assessment with
special focus on cranial nerve function
• Endoscopic assessment of the nasal cavity- to visualize
any nasal lesions and document septal integrity, septal
deviations,and any other anatomical findings.
• A complete ophthalmologic examination & visual fields
examination.
• Signs of intracranial hypertension detected by
papilledema should be addressed preoperatively
[external ventricular drainage (EVD) or
ventriculoperitoneal (VP) shunt ]](https://image.slidesharecdn.com/endoscopicskullbasesurgery-leveliii-151013174420-lva1-app6891/85/Endoscopic-skull-base-surgery-level-iii-8-320.jpg)






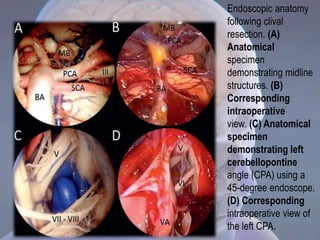
![For intradural exposure, the external layer of the dura is first incised with a No.
11 blade.
Bleeding in the basilar plexus not cauterized but packed with hemostatic
material
The opening of the internal layer of the dura at the level of the middle and
superior clivus must be accomplished with great care to avoid injury to the
underlying basilar artery.
Once the dura opened, minor bleeding is stopped by bipolar coagulation, and
finally the 0-degree endoscope carefully introduced into the intradural space.
Once the anatomy is appreciated, identify the major vessels of the posterior
fossa (basilar artery and branches, anterior inferior cerebellar artery [AICA],
vertebral arteries, superior cerebellar and posterior cerebral arteries); the
intradural course of cranial nerves III, IV, V, and VI; the brainstem; and the
mamillary bodies.
The cerebellopontine angle, cranial nerves VII through XII, and retrosellar
regions are best visualized with the 45-degree endoscope](https://image.slidesharecdn.com/endoscopicskullbasesurgery-leveliii-151013174420-lva1-app6891/85/Endoscopic-skull-base-surgery-level-iii-38-320.jpg)