
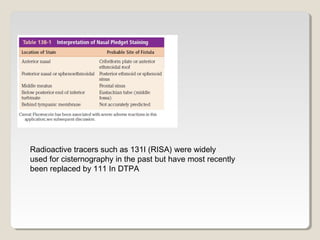
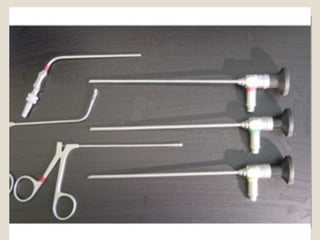
![Light source
Cable
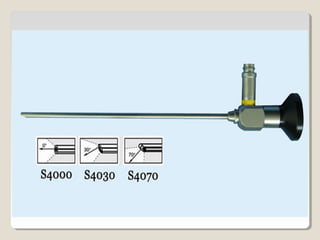
Endoscope [0 - 30 degree] , [wide angle] ,
[2.7 - 4 mm]
Suction tubes [straight - curved]
Forceps [forward - upward]](https://image.slidesharecdn.com/endoscopicnasalanatomy-190425083125/85/Endoscopic-nasal-anatomy-83-320.jpg)

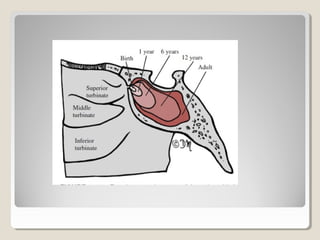
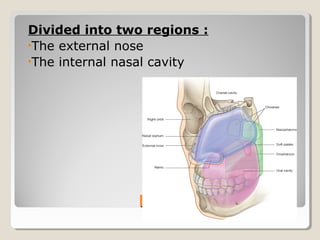
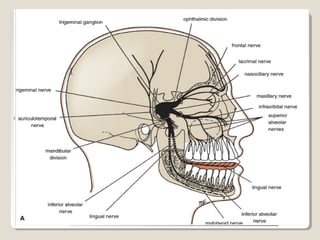
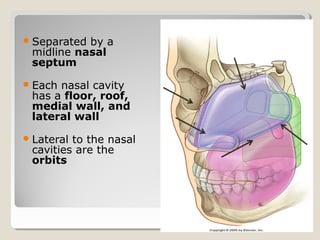
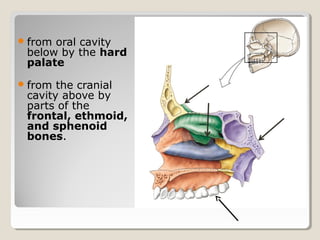
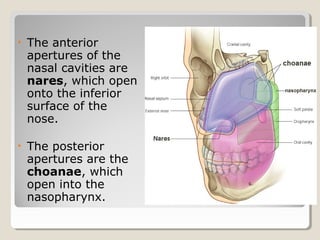
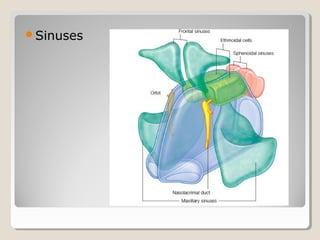
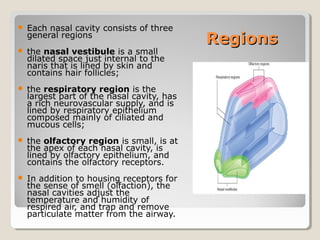
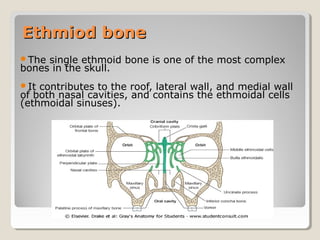
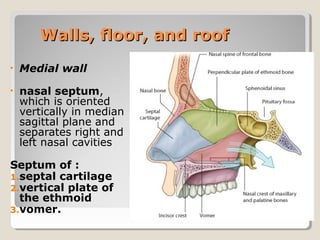
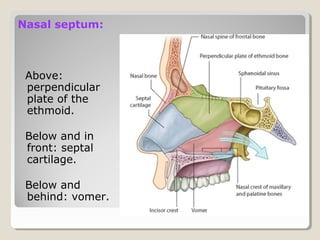
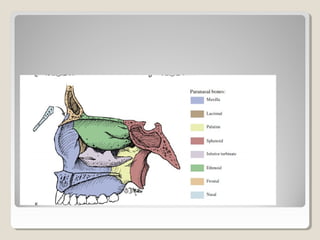
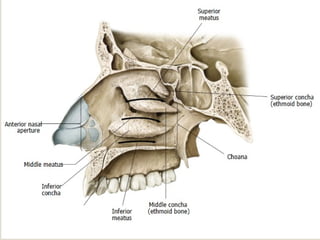
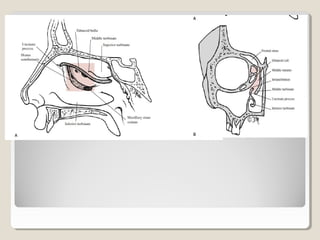
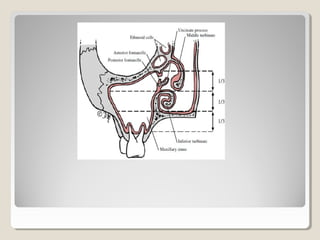
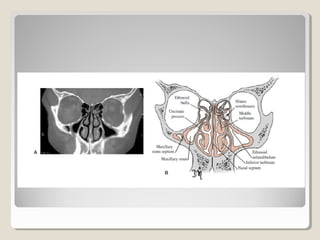
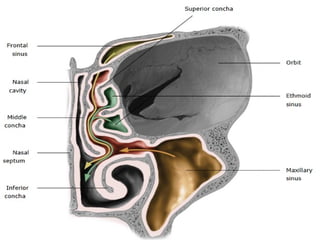
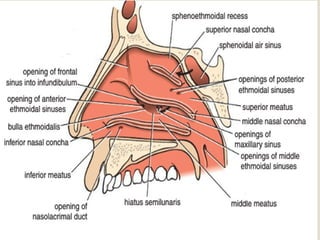
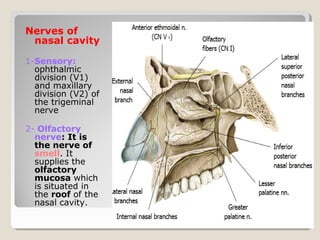
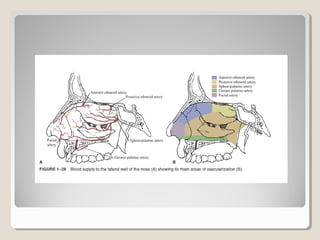
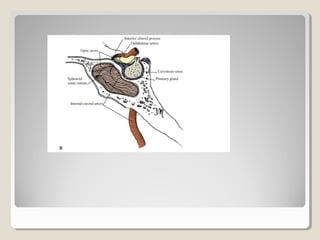
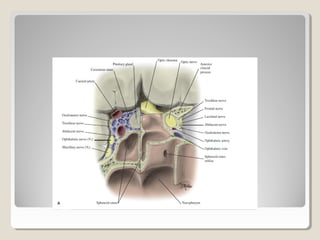
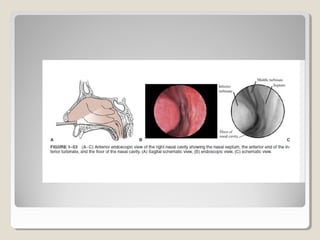
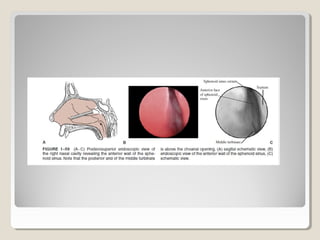
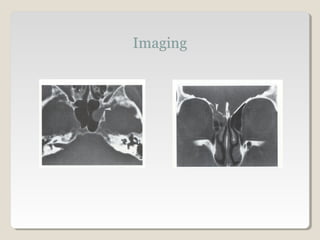
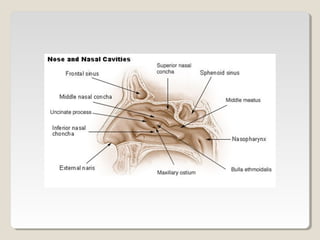
The nasal cavity and paranasal sinuses have a complex anatomy. The nasal cavity is divided into two regions by the nasal septum and has three main regions - the nasal vestibule, respiratory region, and olfactory region. It is bounded by the nasal bones, ethmoid bone, maxillae, palatine bones, lacrimal bones and sphenoid bones. The paranasal sinuses include the frontal, ethmoid, maxillary and sphenoid sinuses. Cerebrospinal fluid leaks can be diagnosed using tests like beta-2 transferrin, CT scans and intrathecal fluorescein. They are usually repaired endoscopically using grafts, tissue adhesives and






























































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)




![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)







