Downloaded 1,882 times

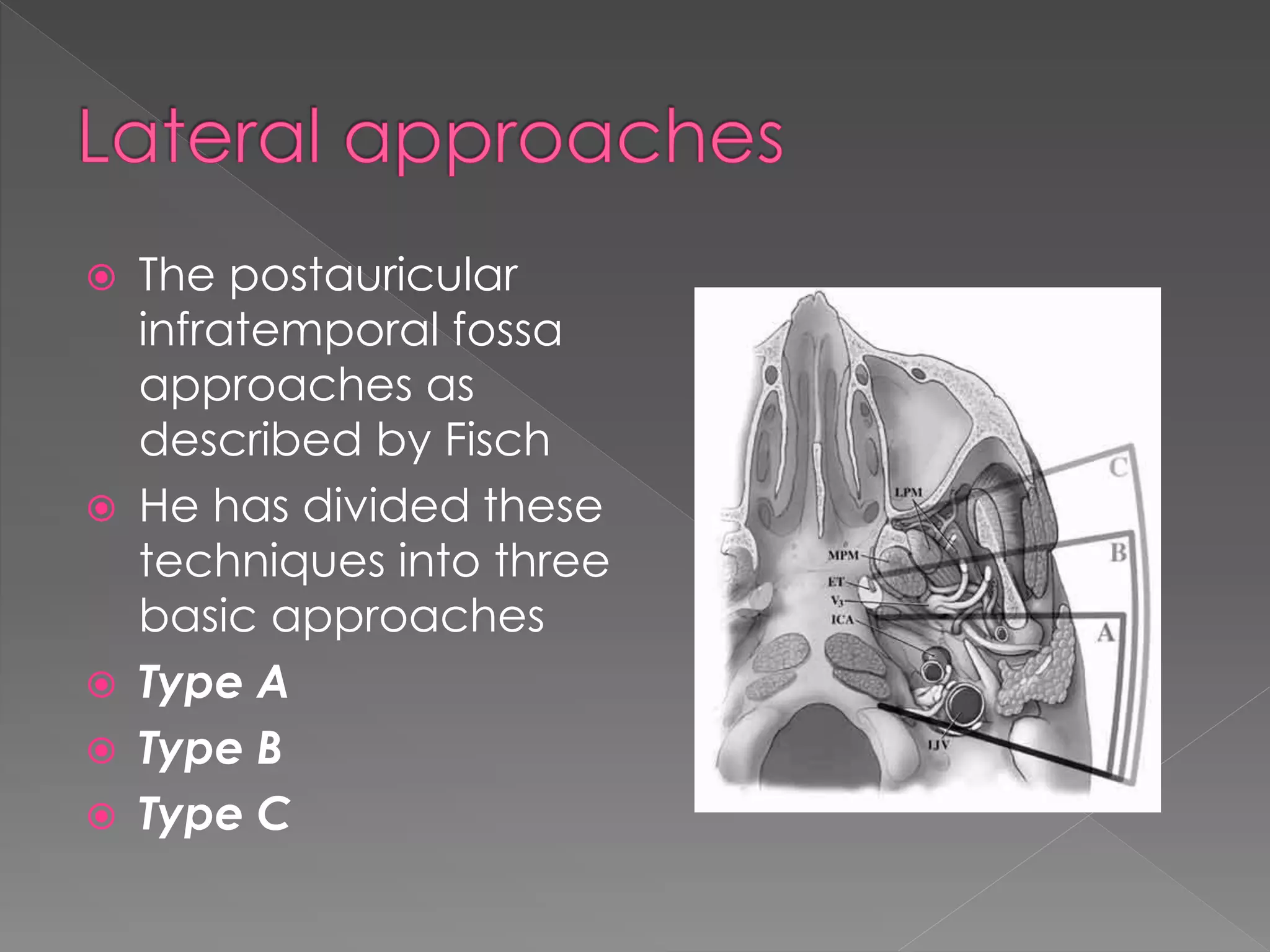







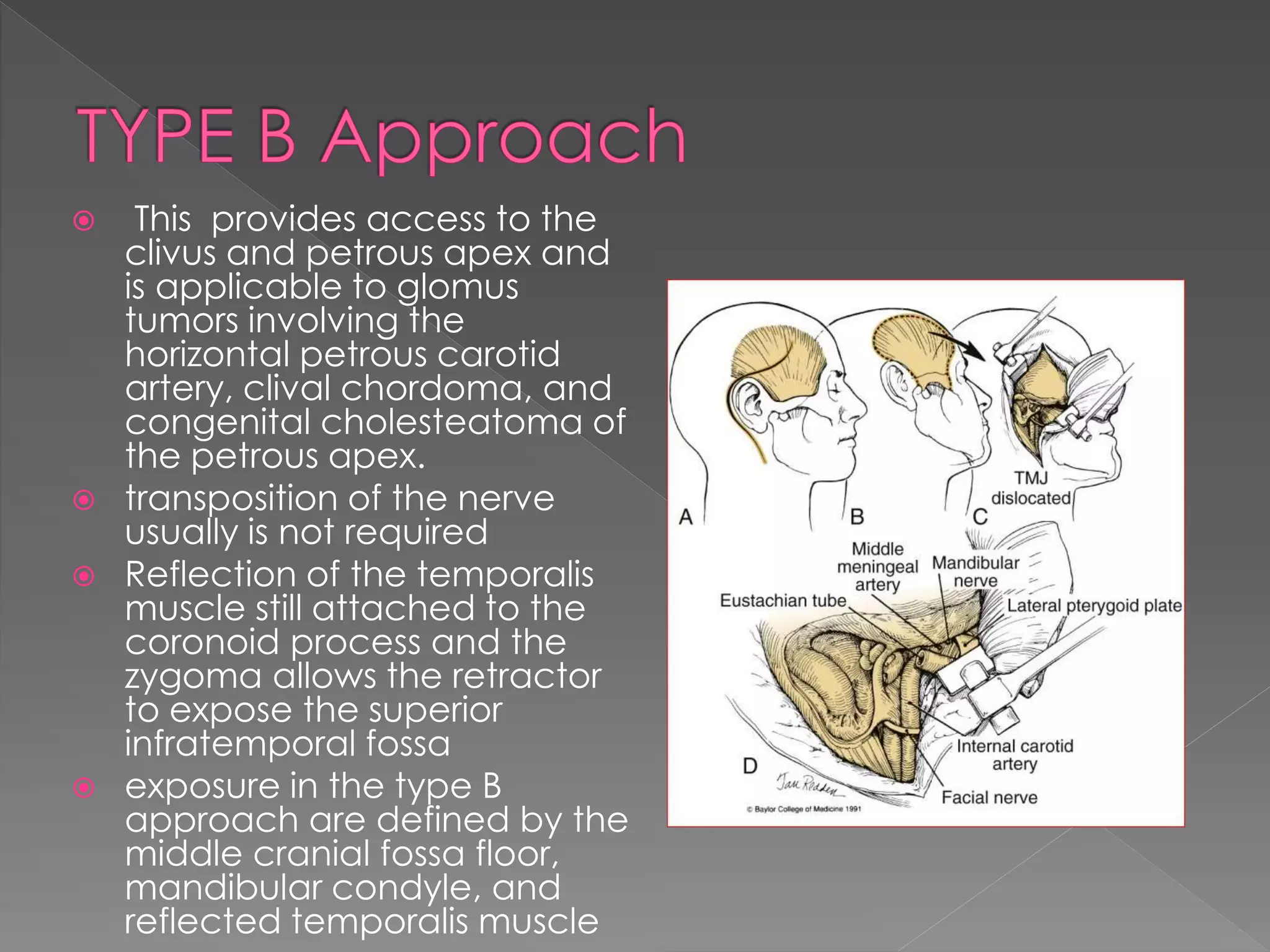




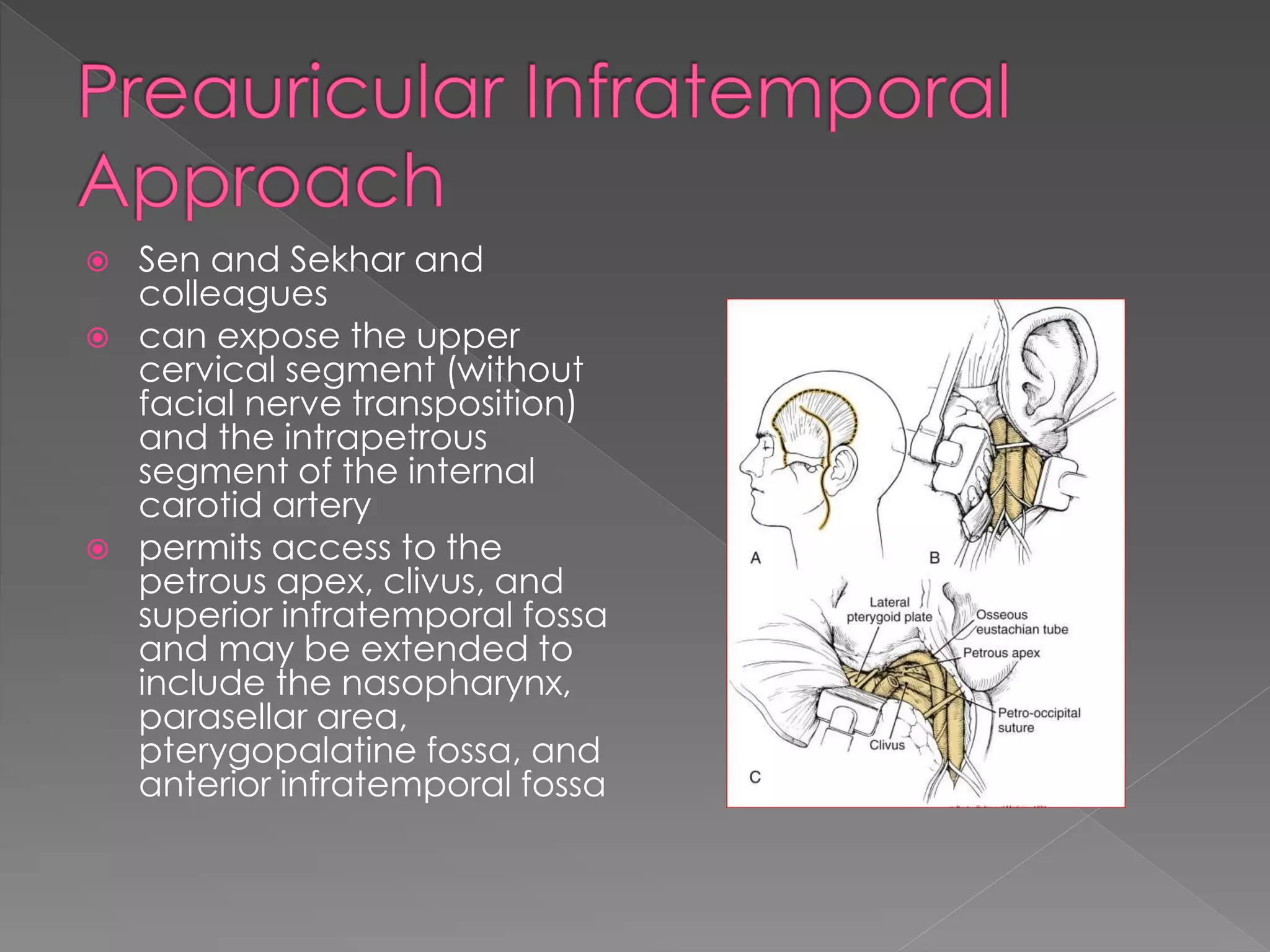




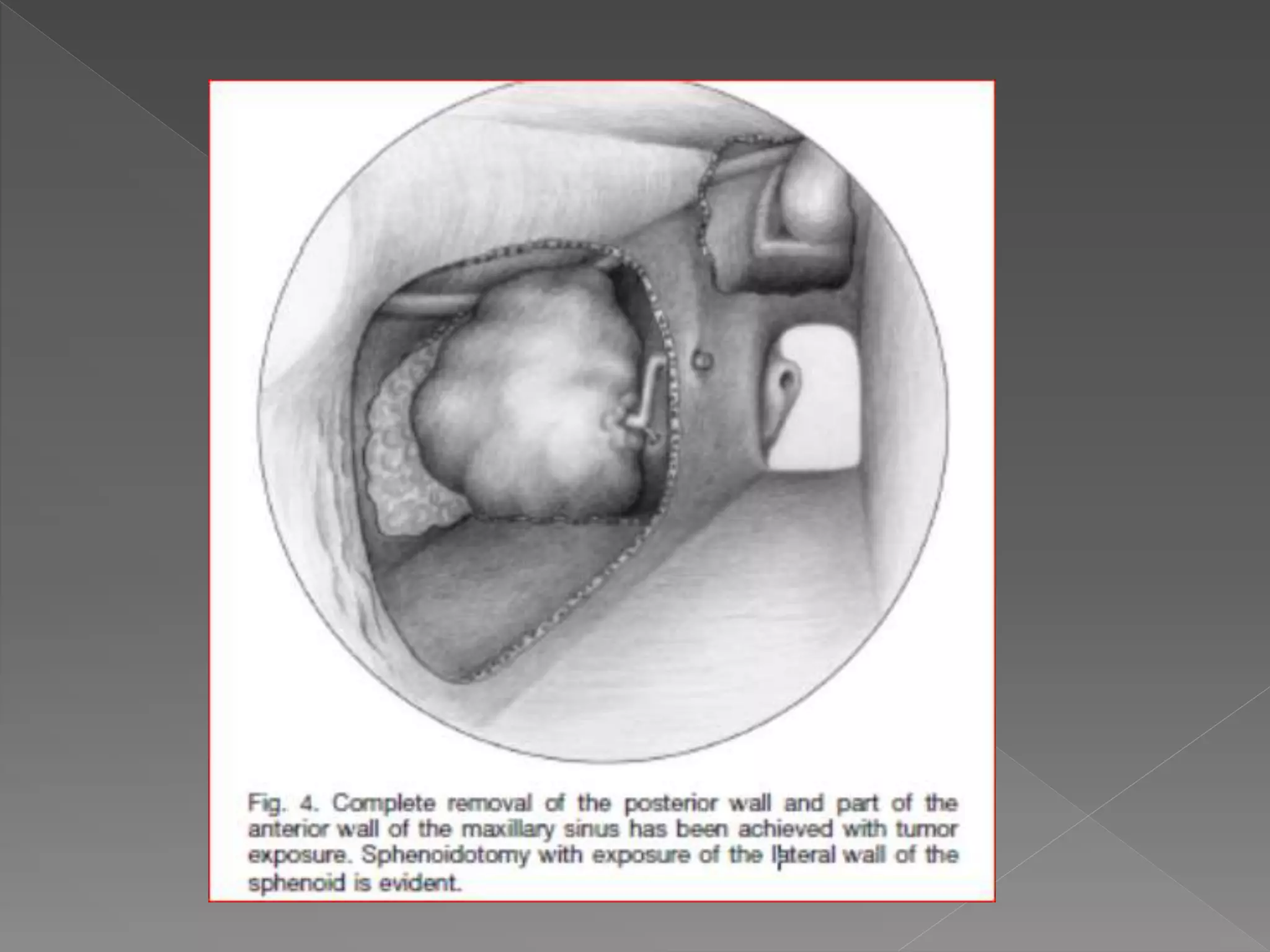







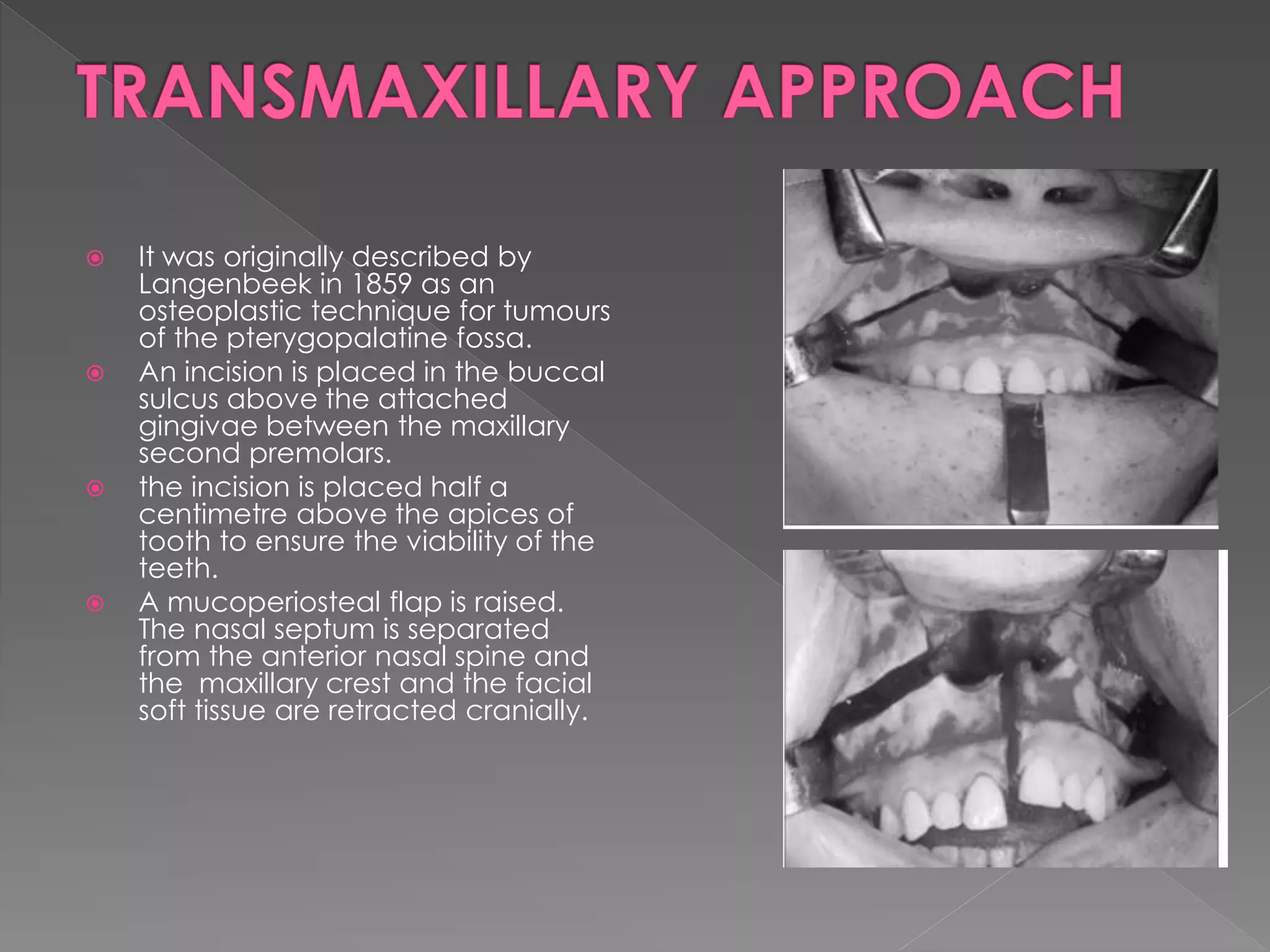






This document describes various approaches to the infratemporal fossa (ITF) for tumors. It discusses anterior approaches like transoral, transantral, and transmaxillary which provide access to the anteromedial ITF. Lateral approaches like transzygomatic access the lateral ITF. Inferior approaches like transmandibular reach the ITF from below. The document outlines the pioneers who developed different ITF approaches and describes in detail the postauricular infratemporal fossa approach developed by Fisch, involving types A, B, and C. It discusses the advantages, disadvantages, and variations of different ITF approaches.






























































































