Downloaded 74 times


















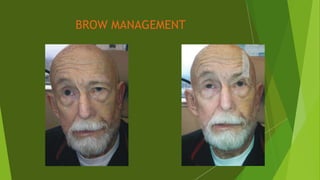




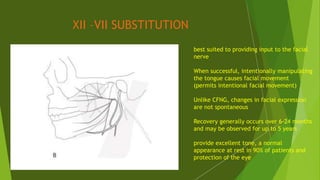






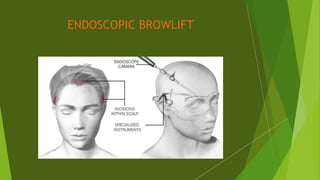




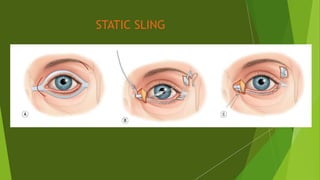




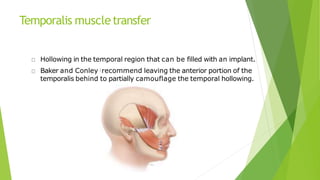
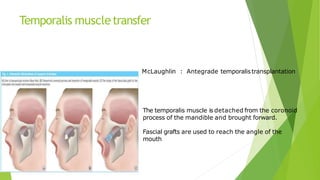





The document discusses facial nerve palsy and facial reanimation. It begins with an introduction to the facial nerve and its functions. It then covers anatomy of the facial nerve, classifications and etiologies of facial nerve palsy, presentation and evaluation, non-surgical and surgical management options. For surgical management it discusses various nerve repair techniques including cable grafting and nerve transfers. It also covers approaches to managing specific areas like the eyebrow, eyelids, and lips which may be paralyzed. Both static and dynamic reconstruction techniques are outlined.


























































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
















![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)