Downloaded 3,689 times




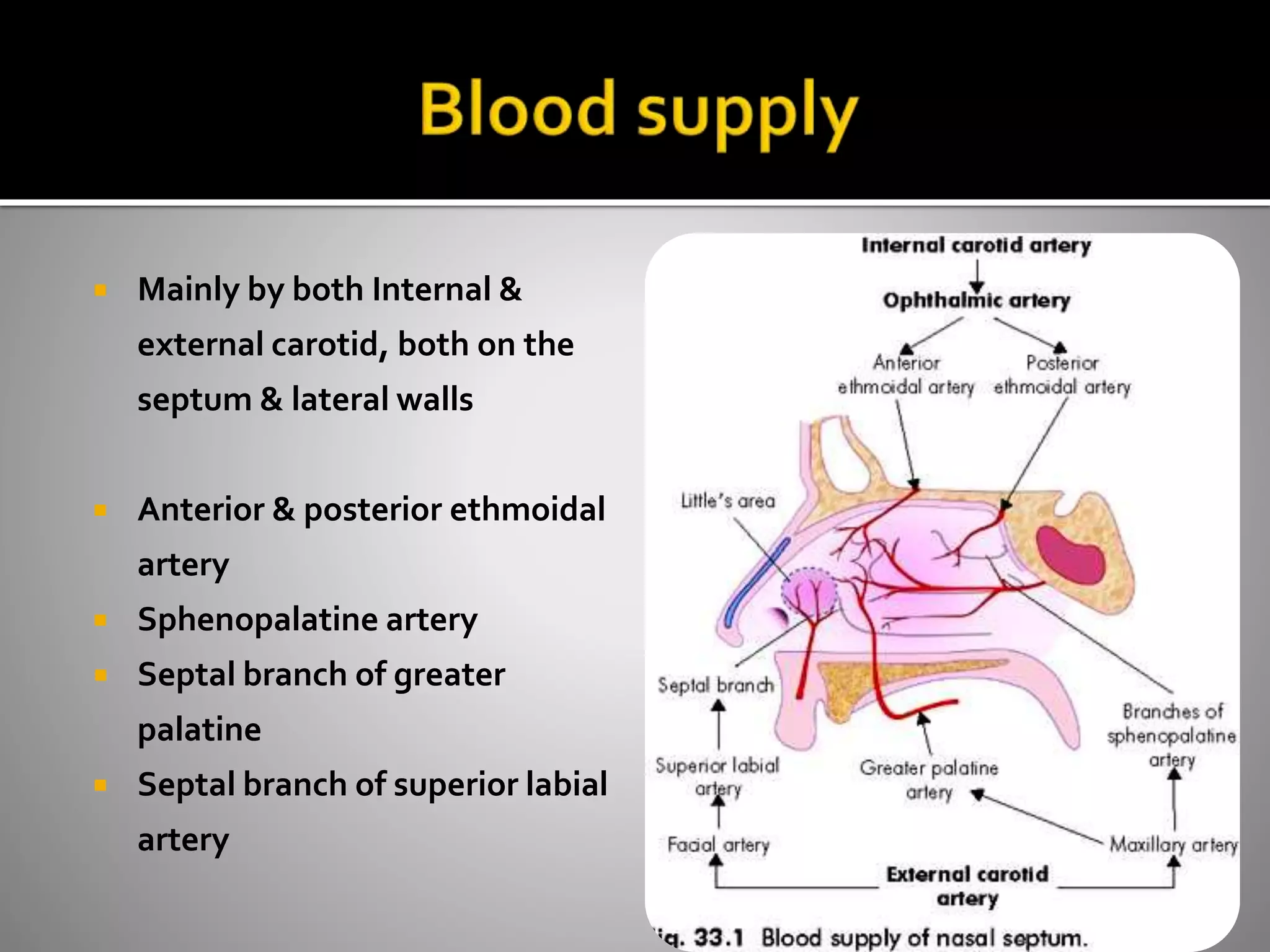






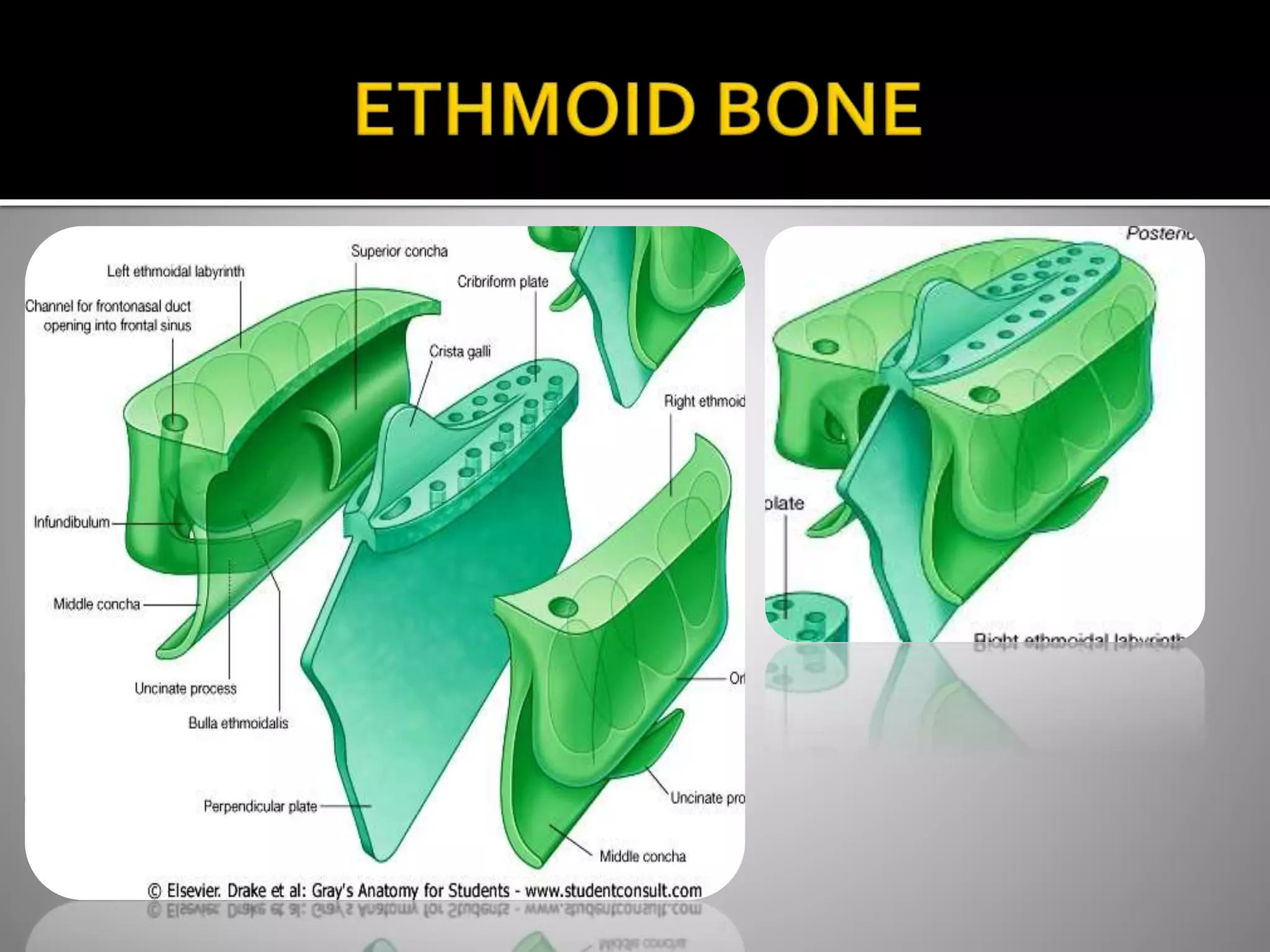



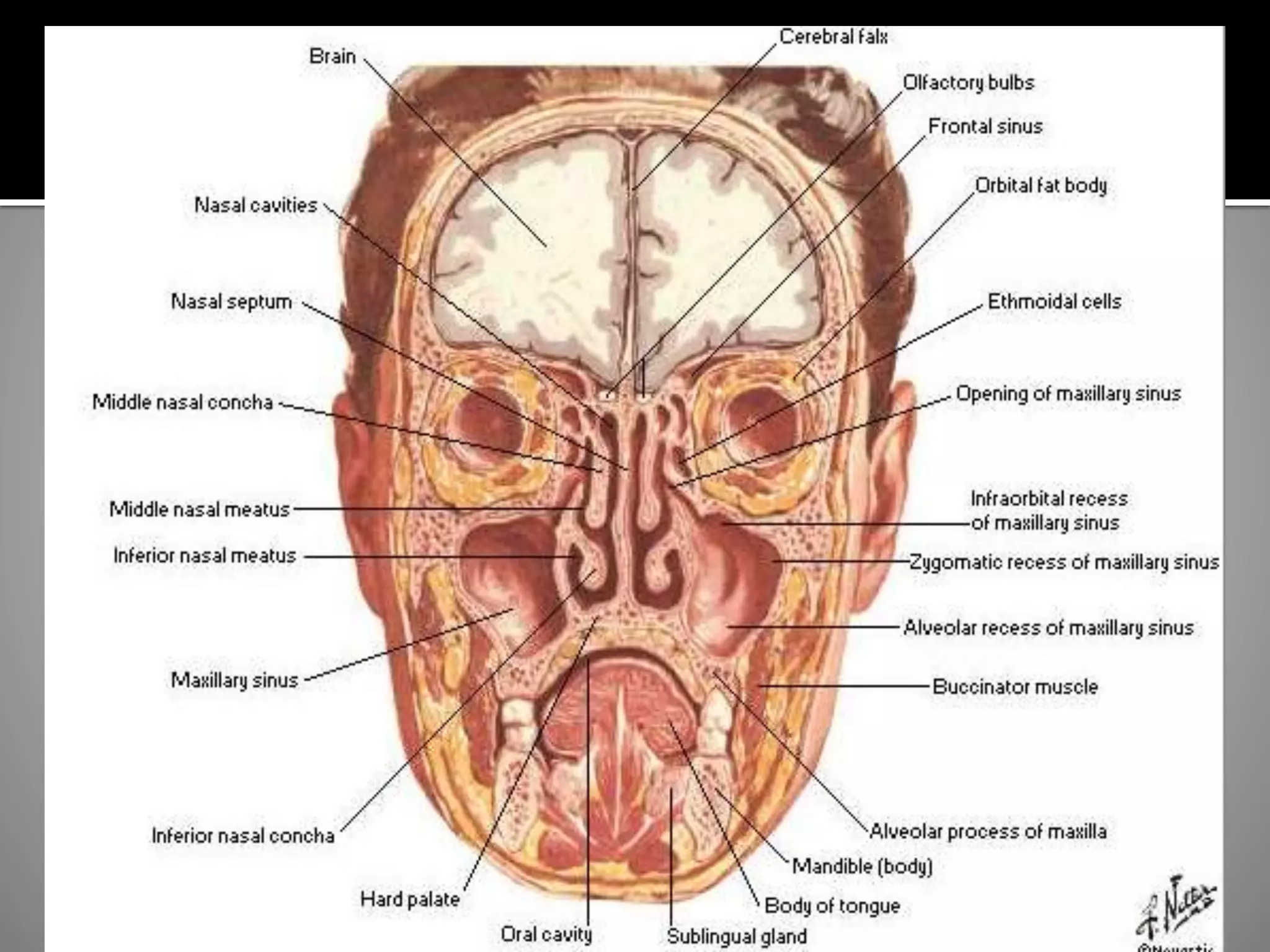








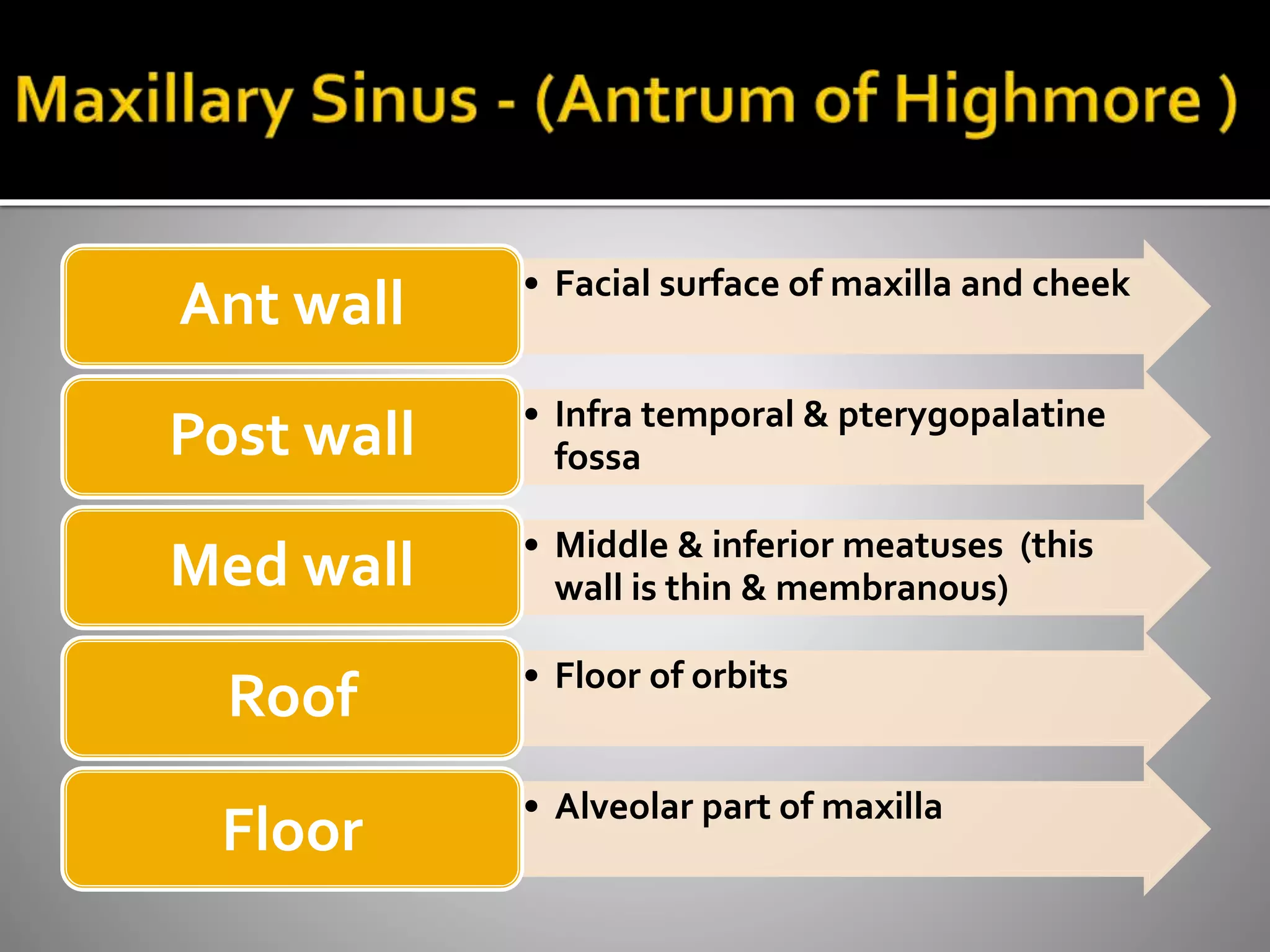



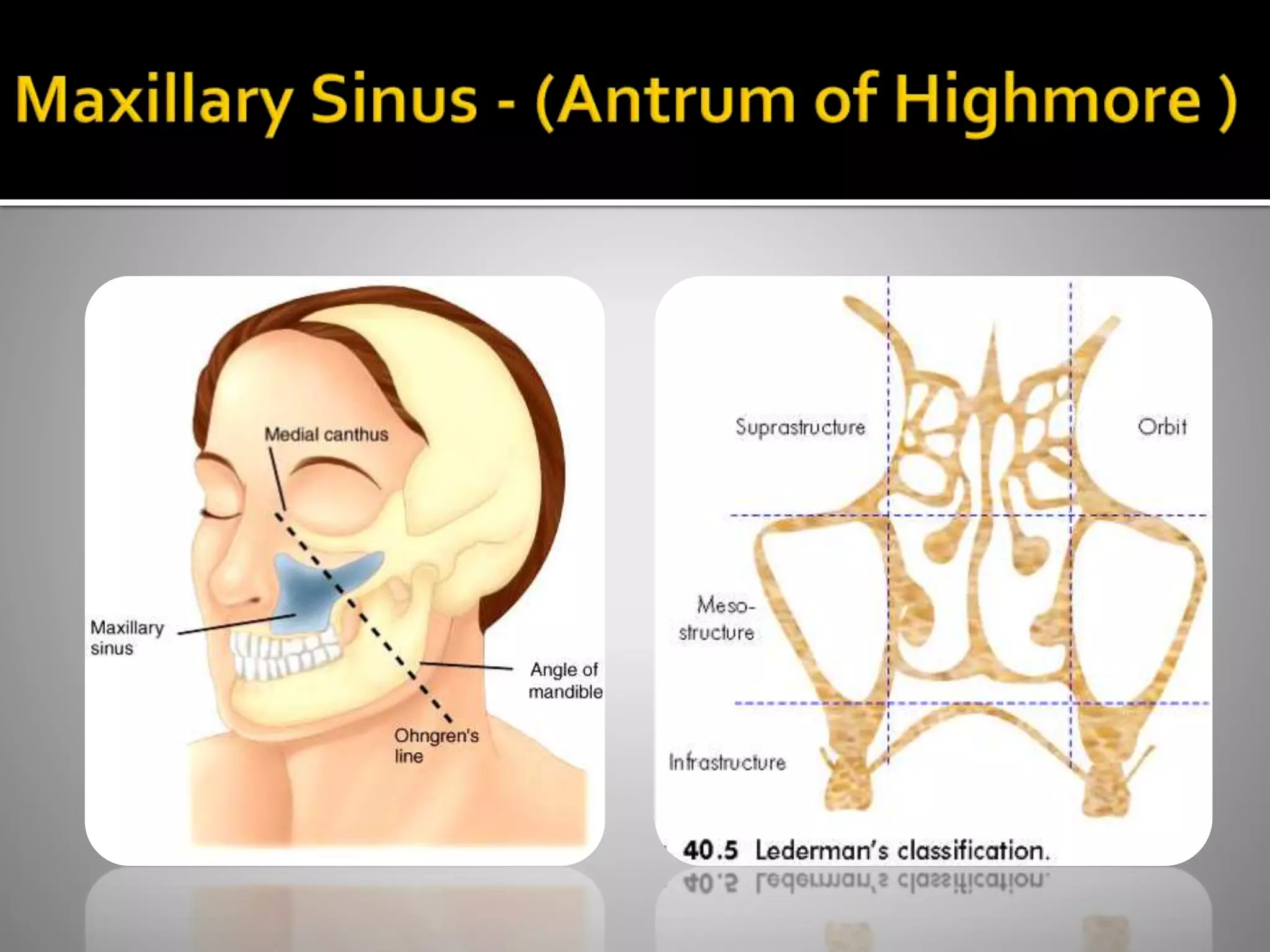












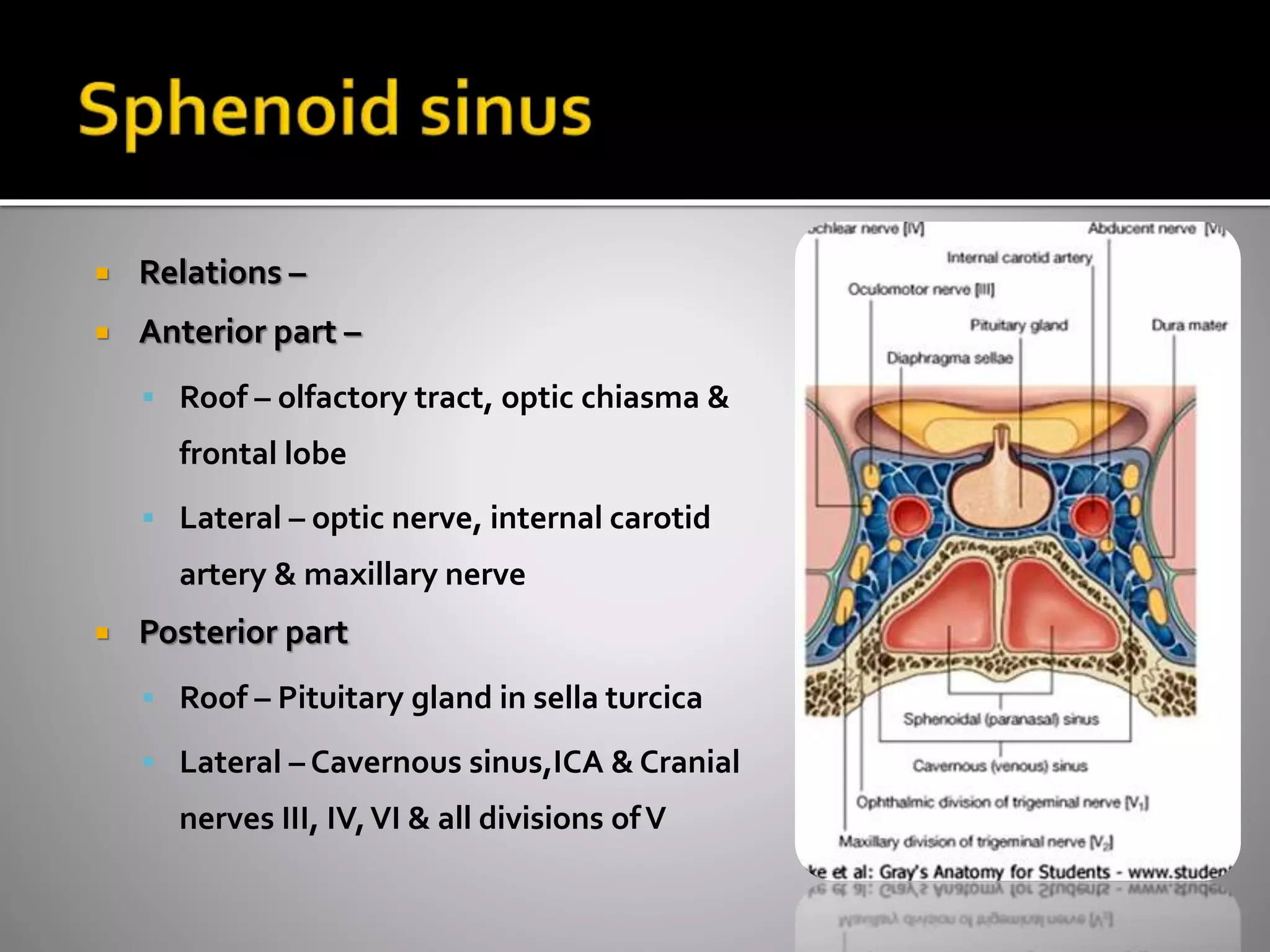





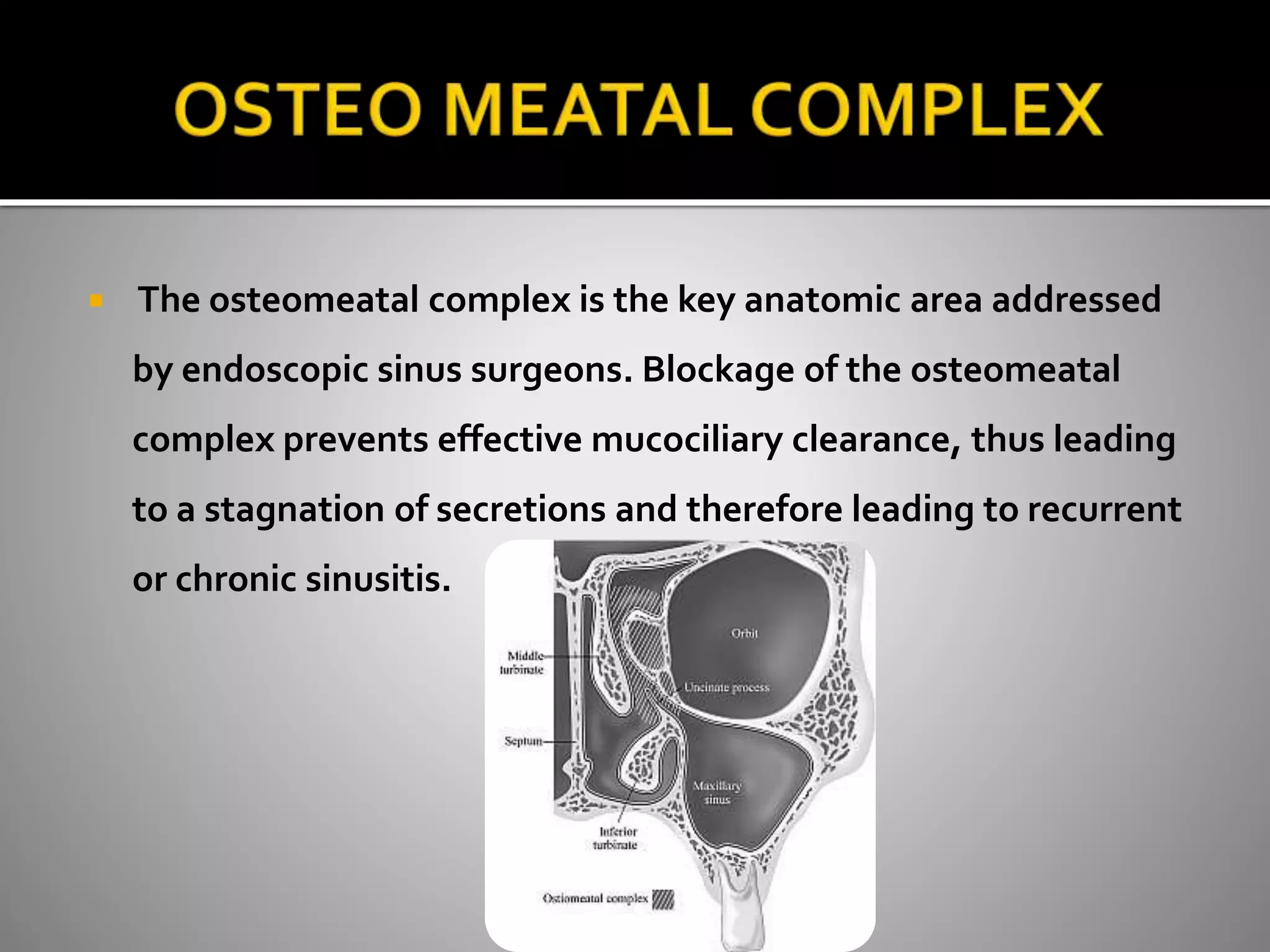
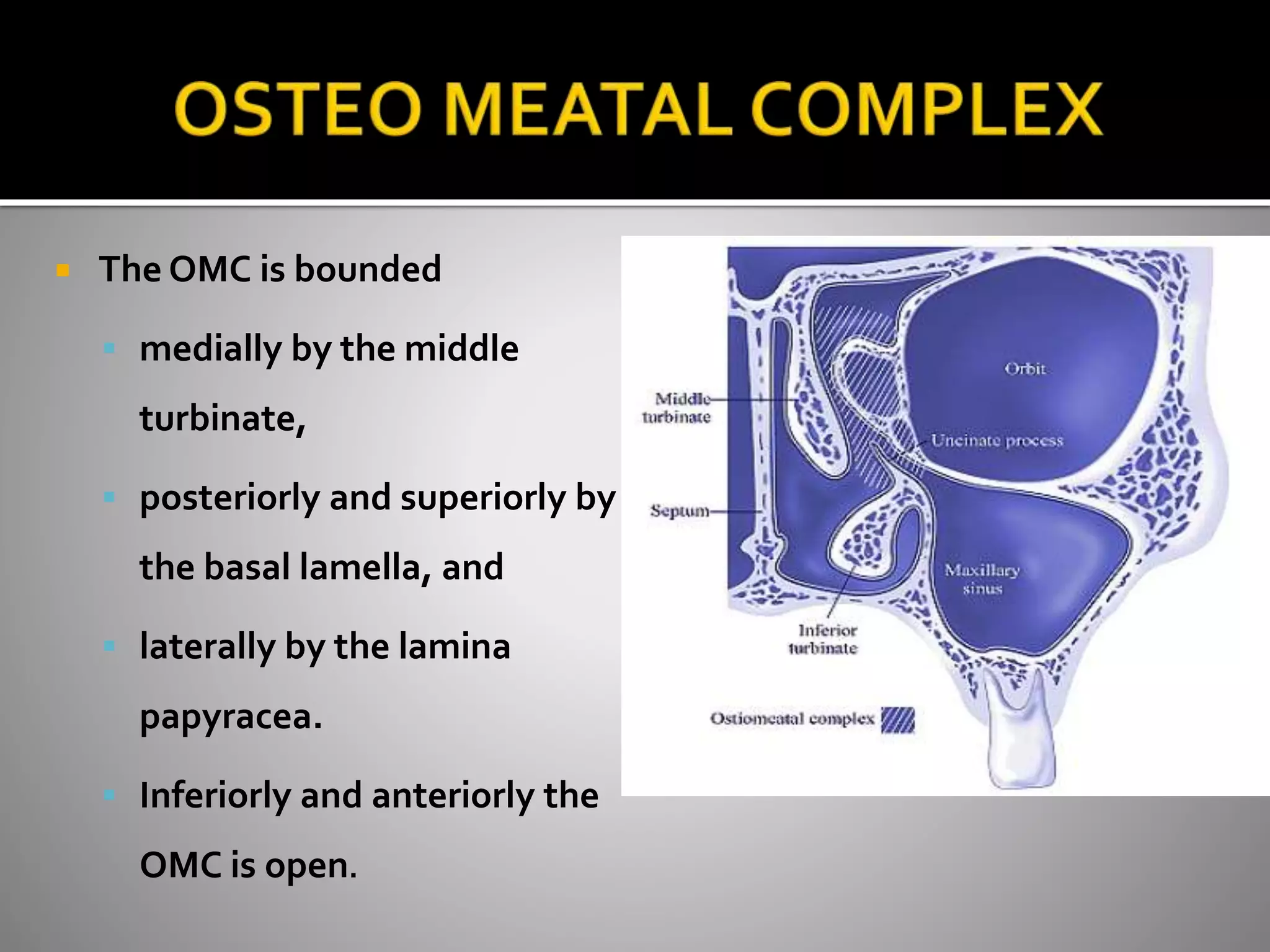











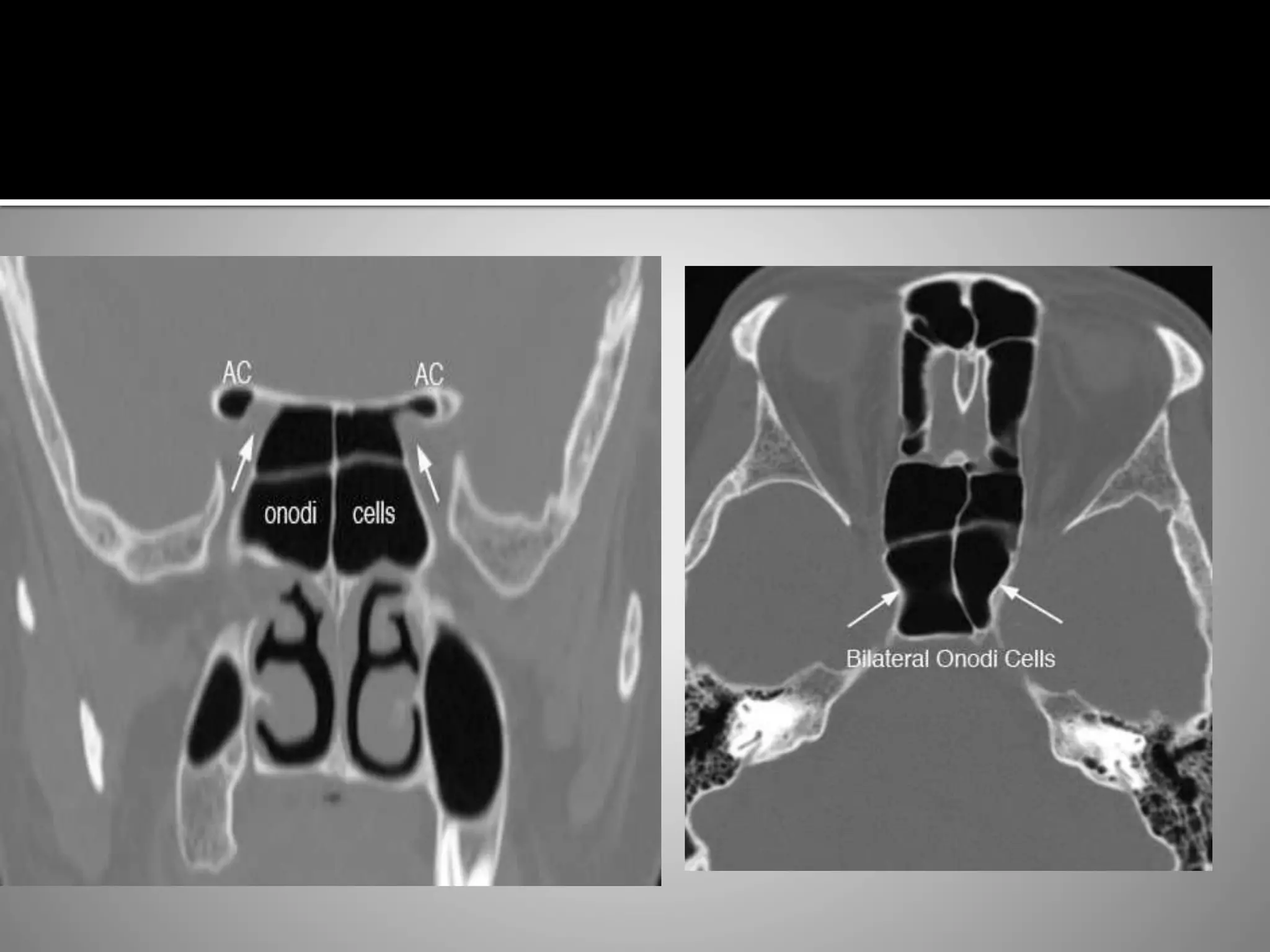






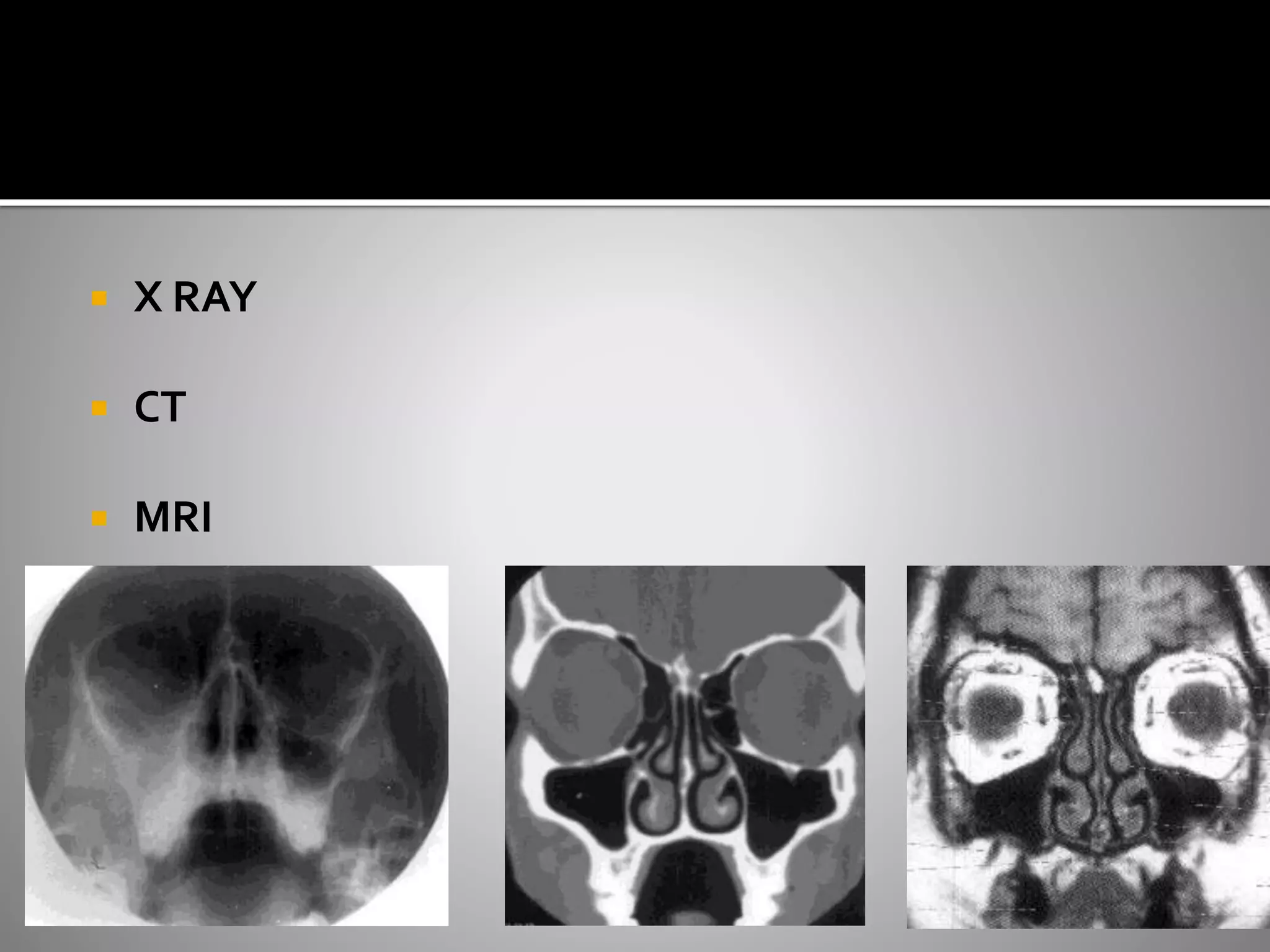













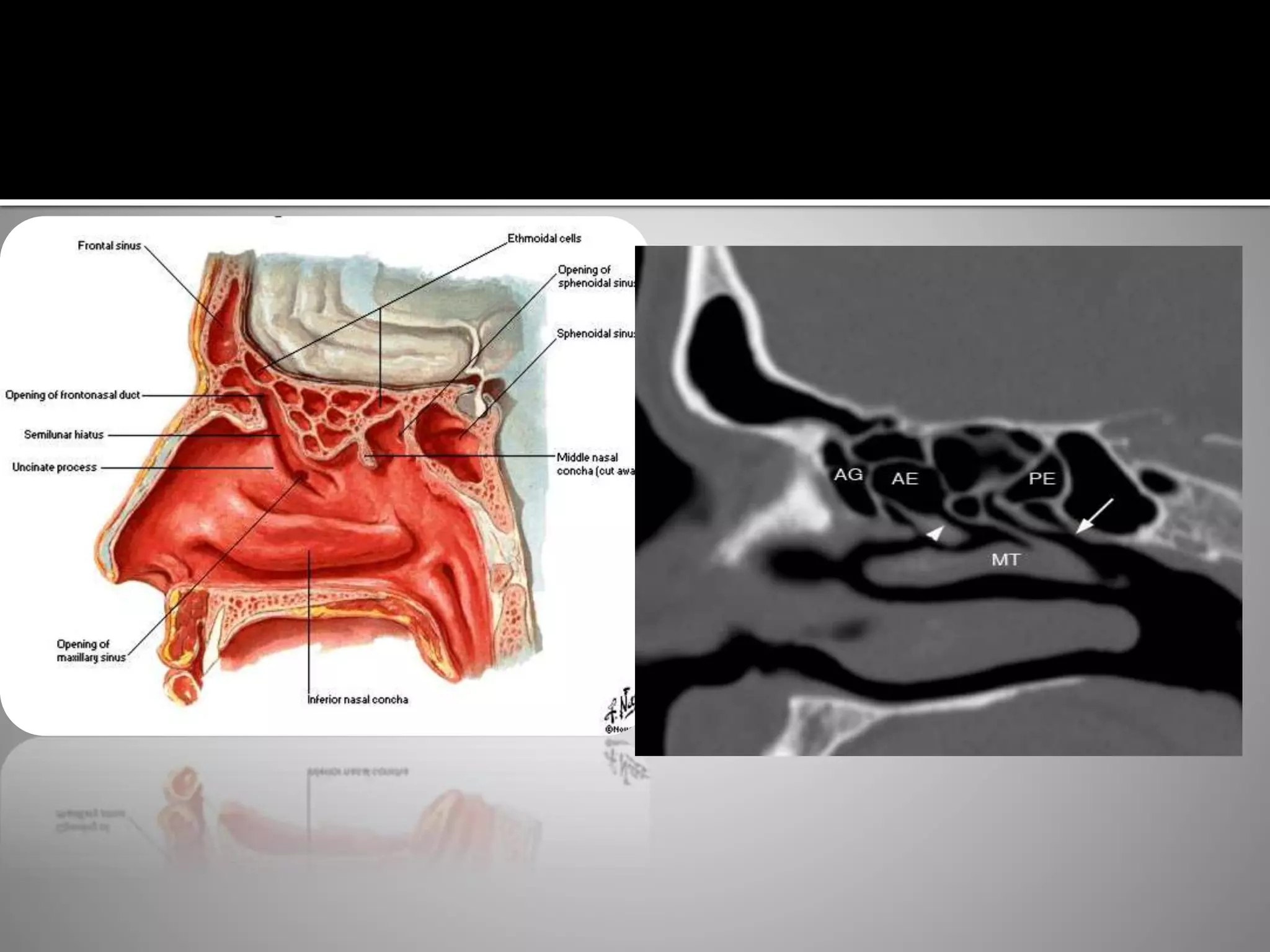





The document provides a detailed overview of the anatomy, variations, and imaging of the nose, nasal fossa, and paranasal sinuses, emphasizing the significance of the osteomeatal complex in diagnosing sinus conditions. It outlines the various anatomical features, developmental stages of the sinuses, and common variations that may affect sinus drainage and health. Diverse imaging modalities, particularly CT scans, are discussed as vital tools for assessing the paranasal sinuses and their related structures.