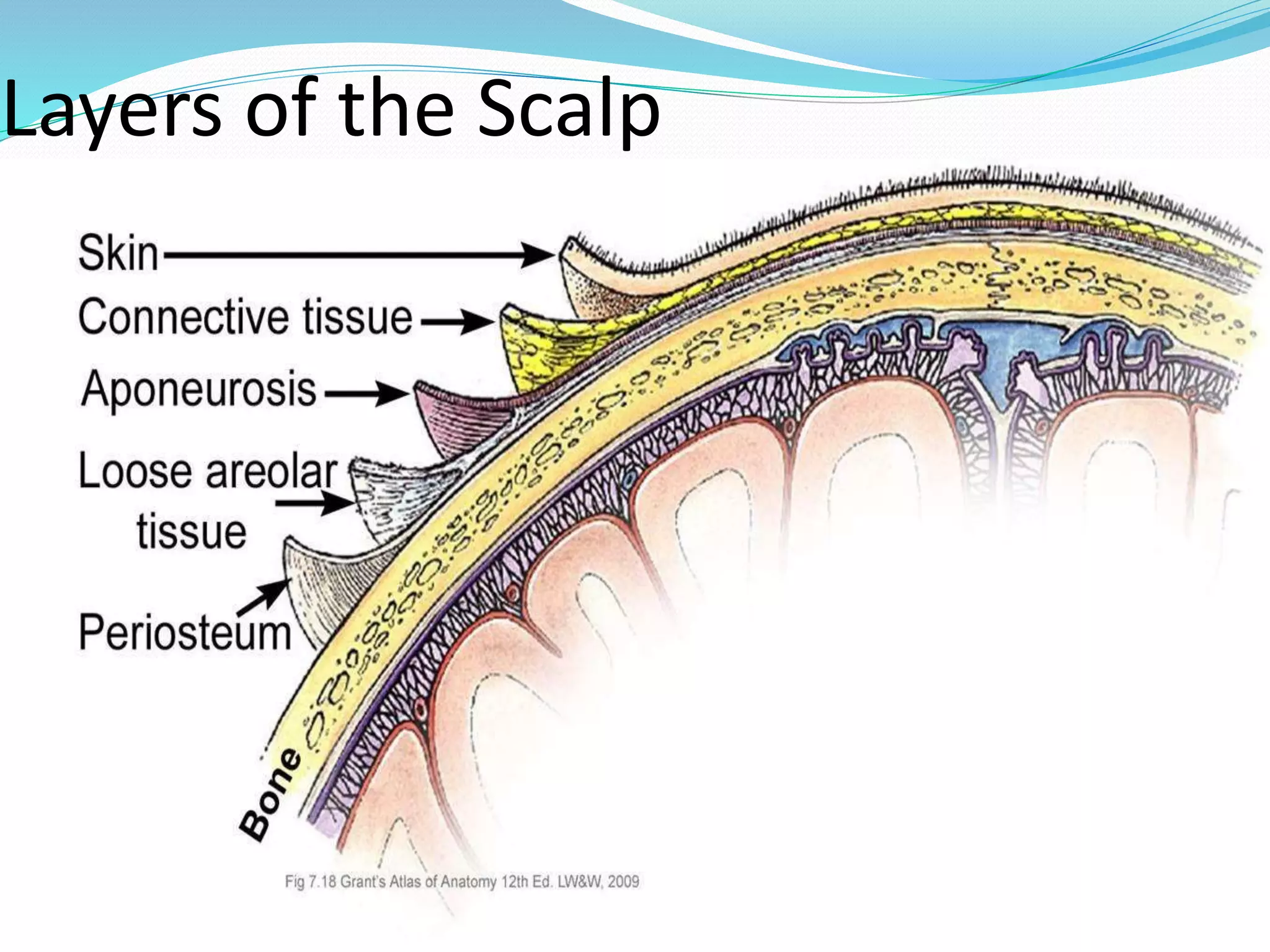
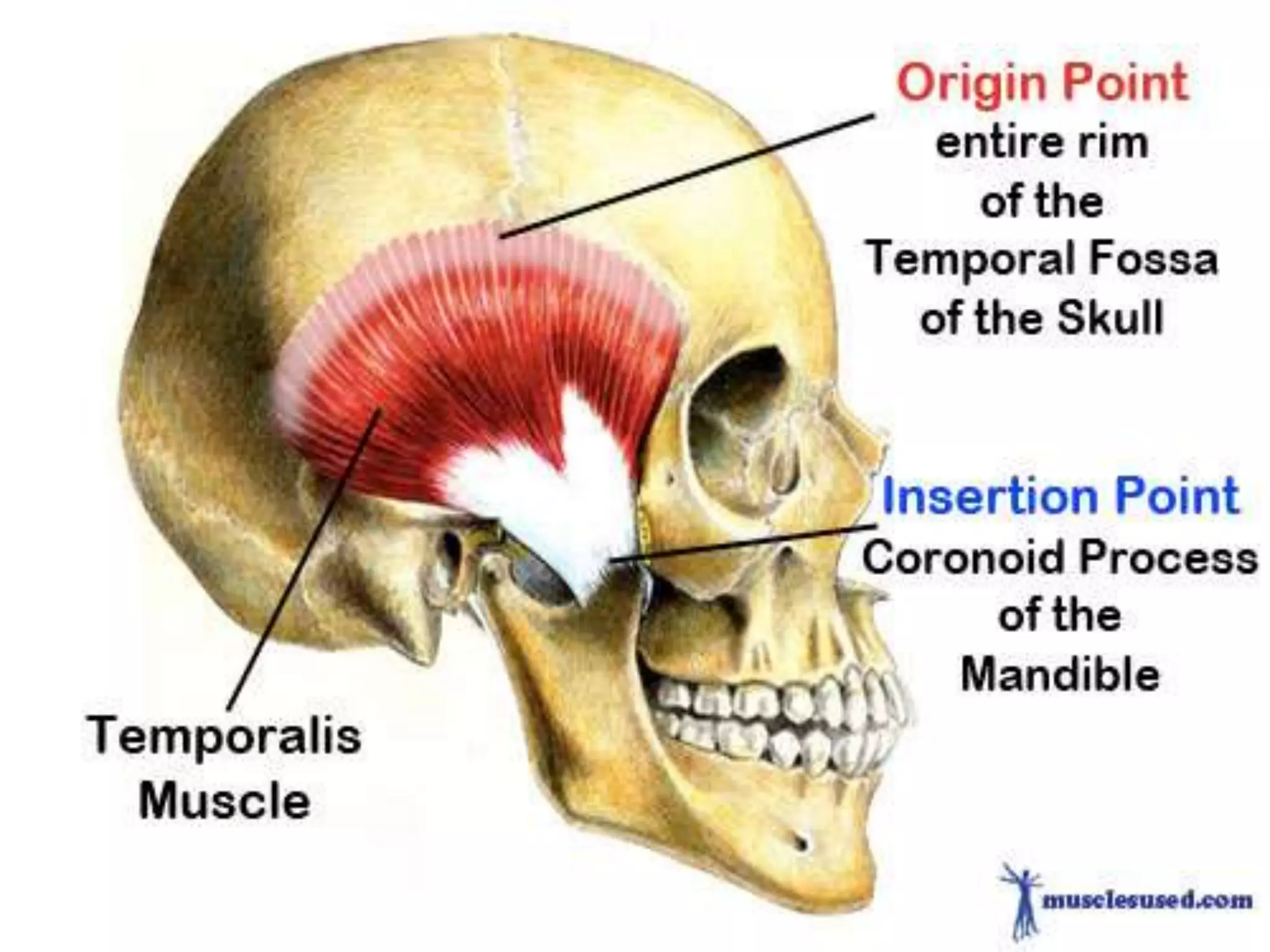
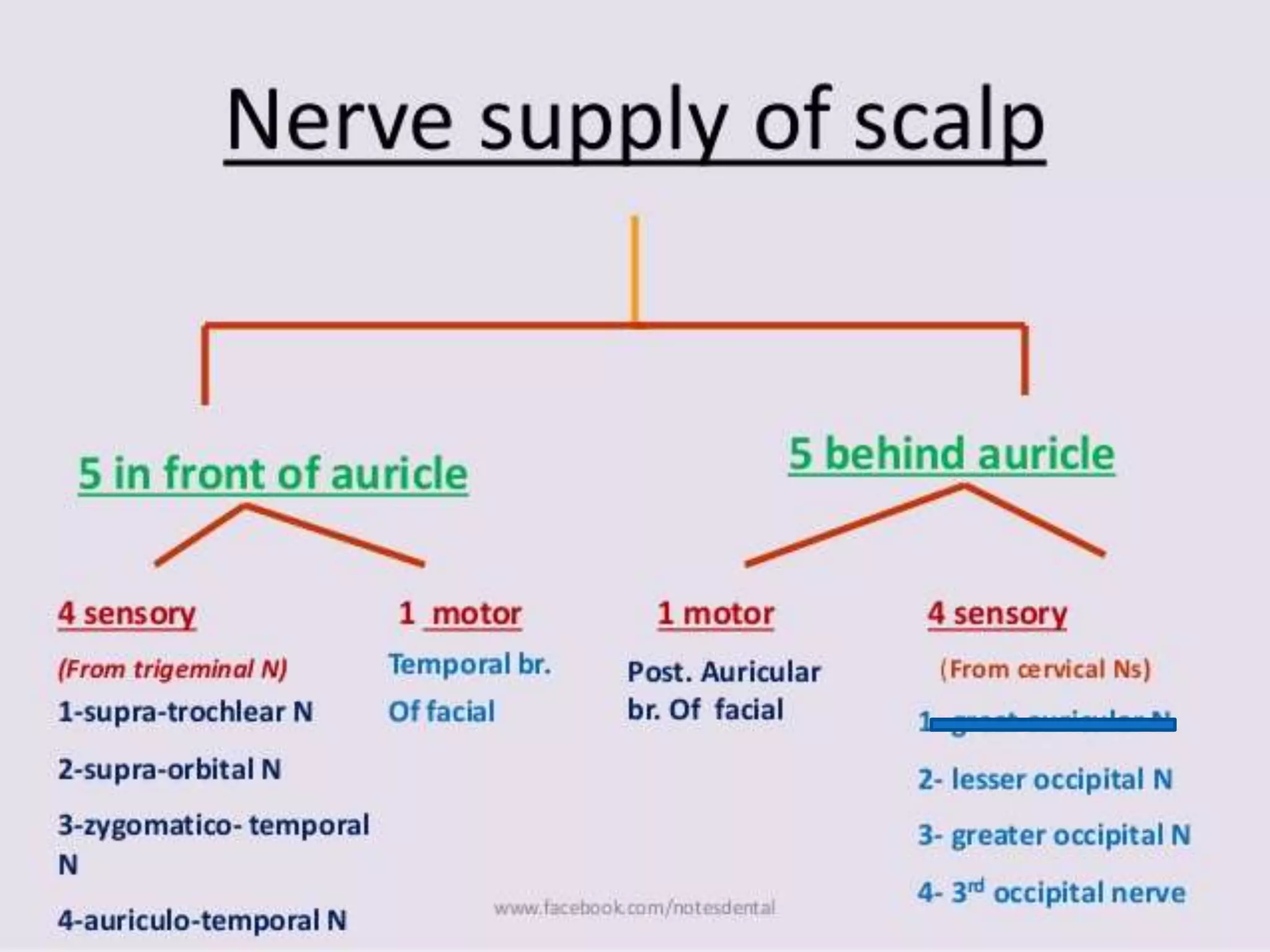
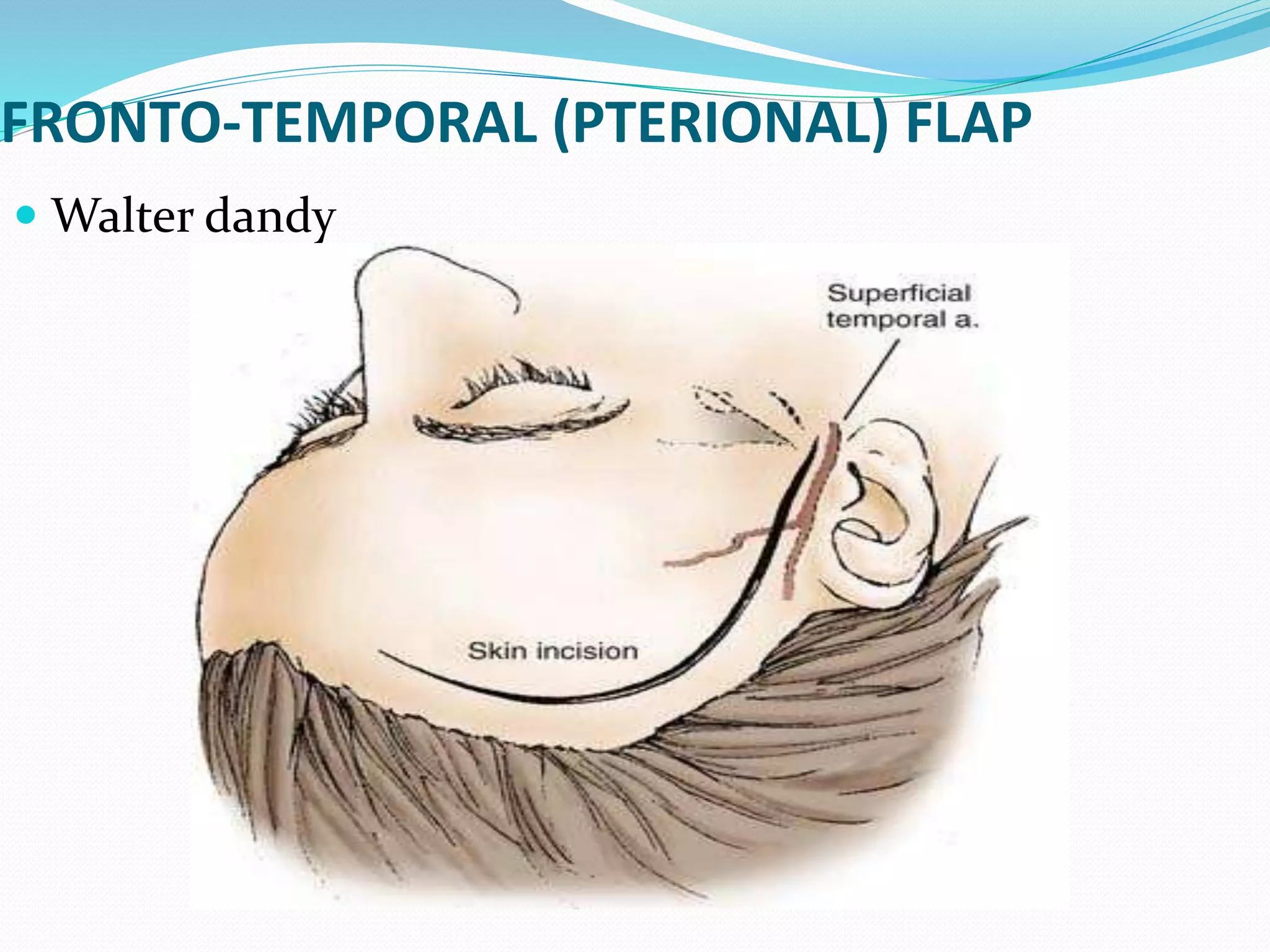
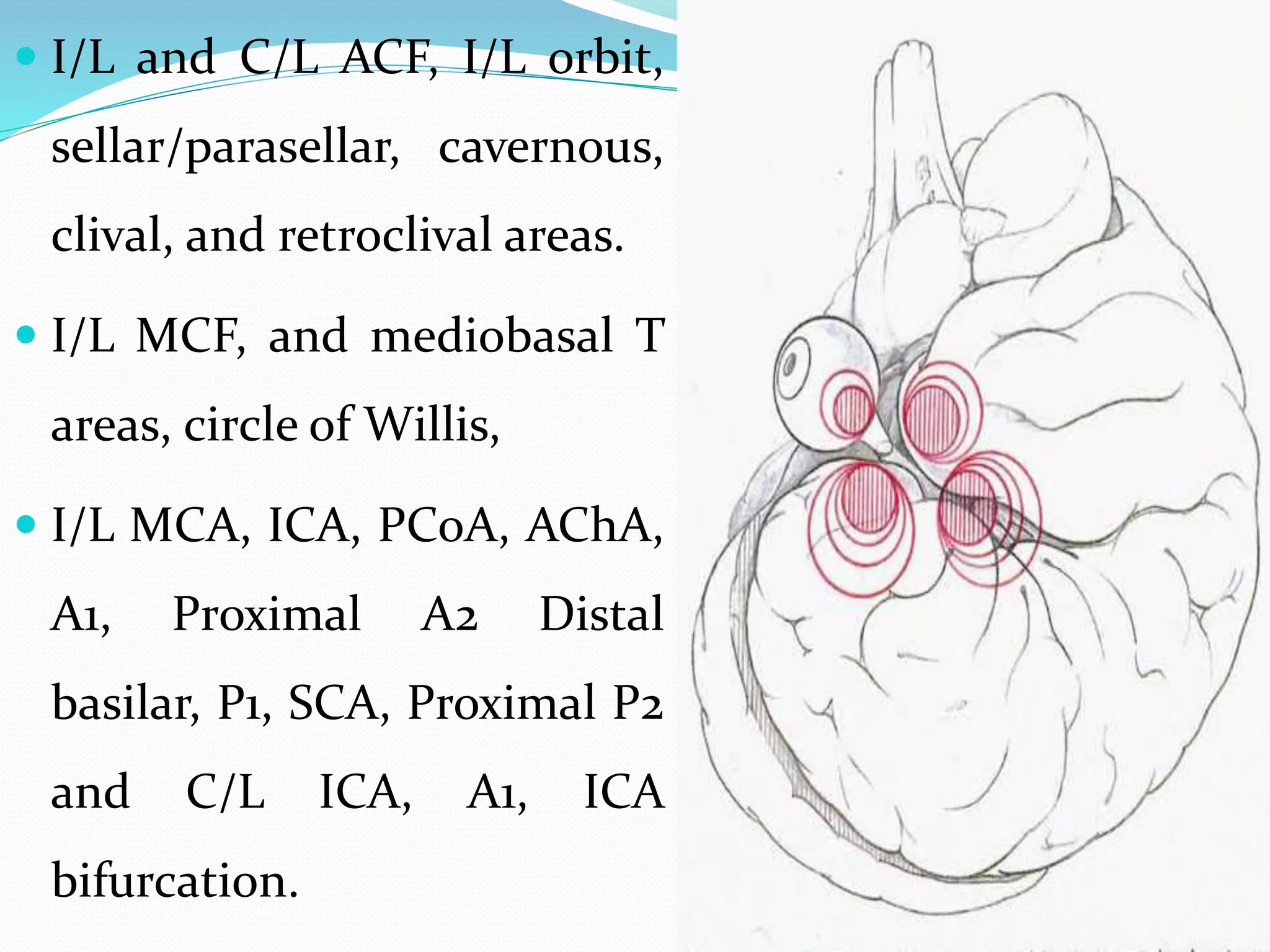
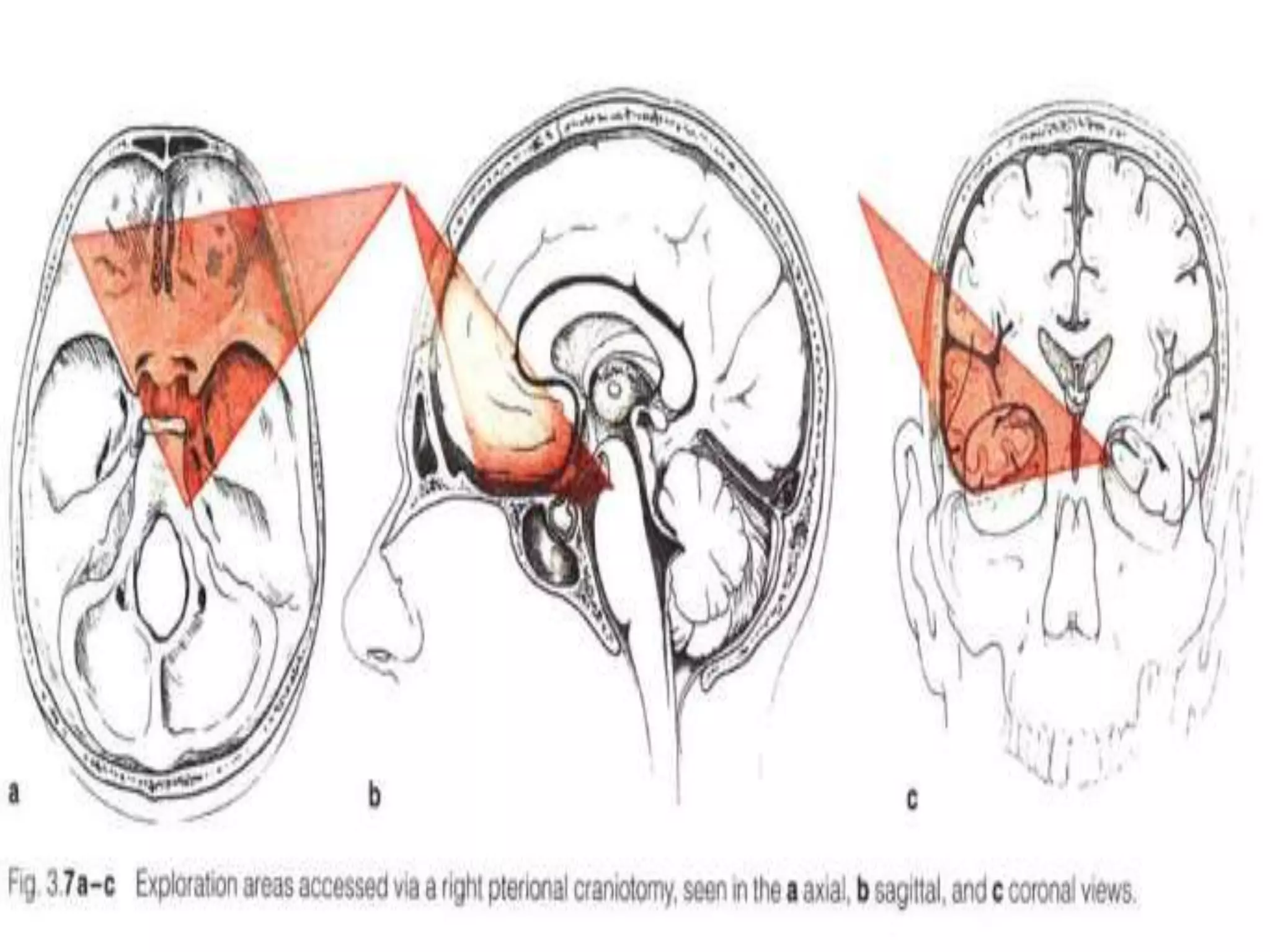
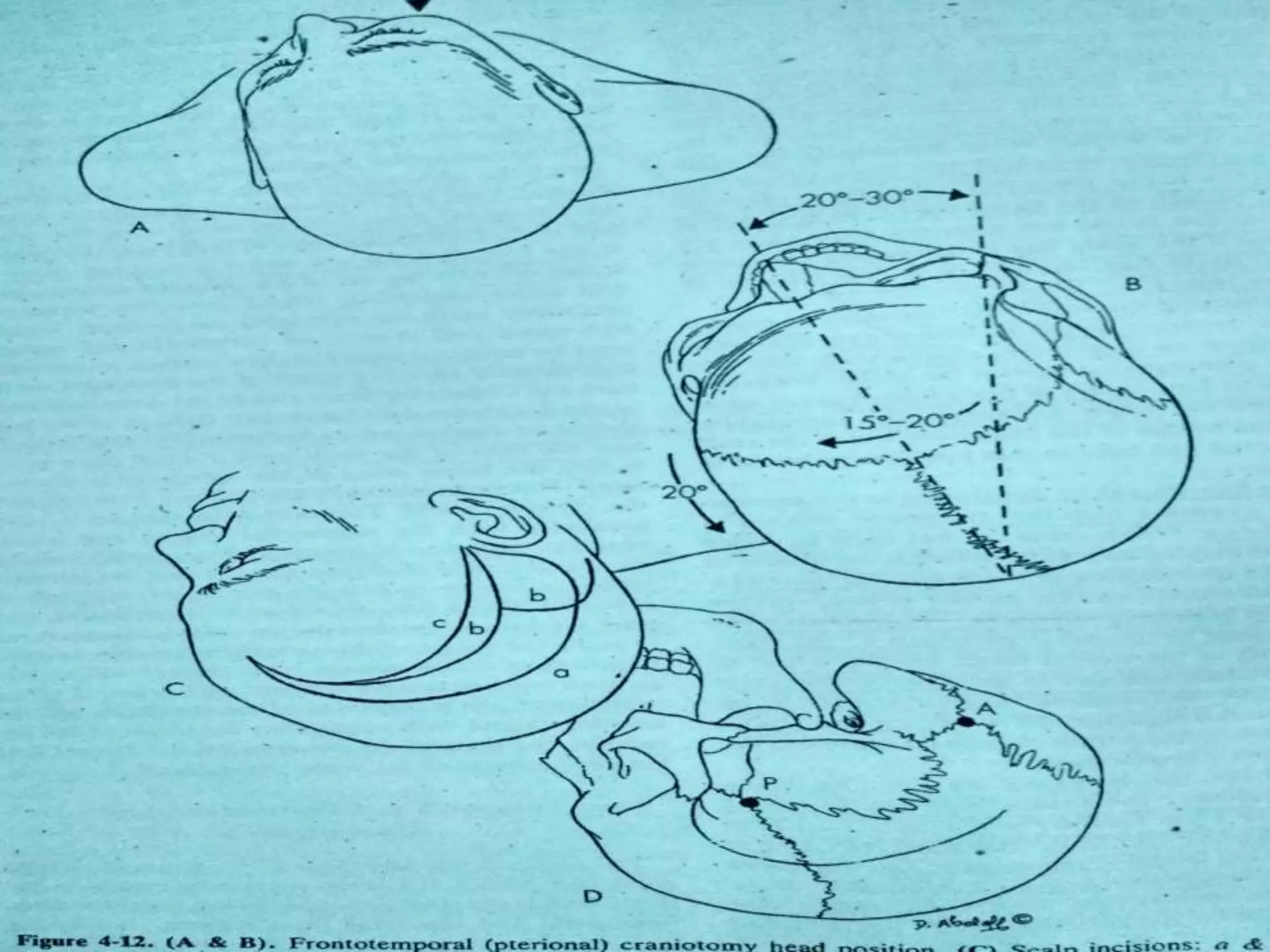
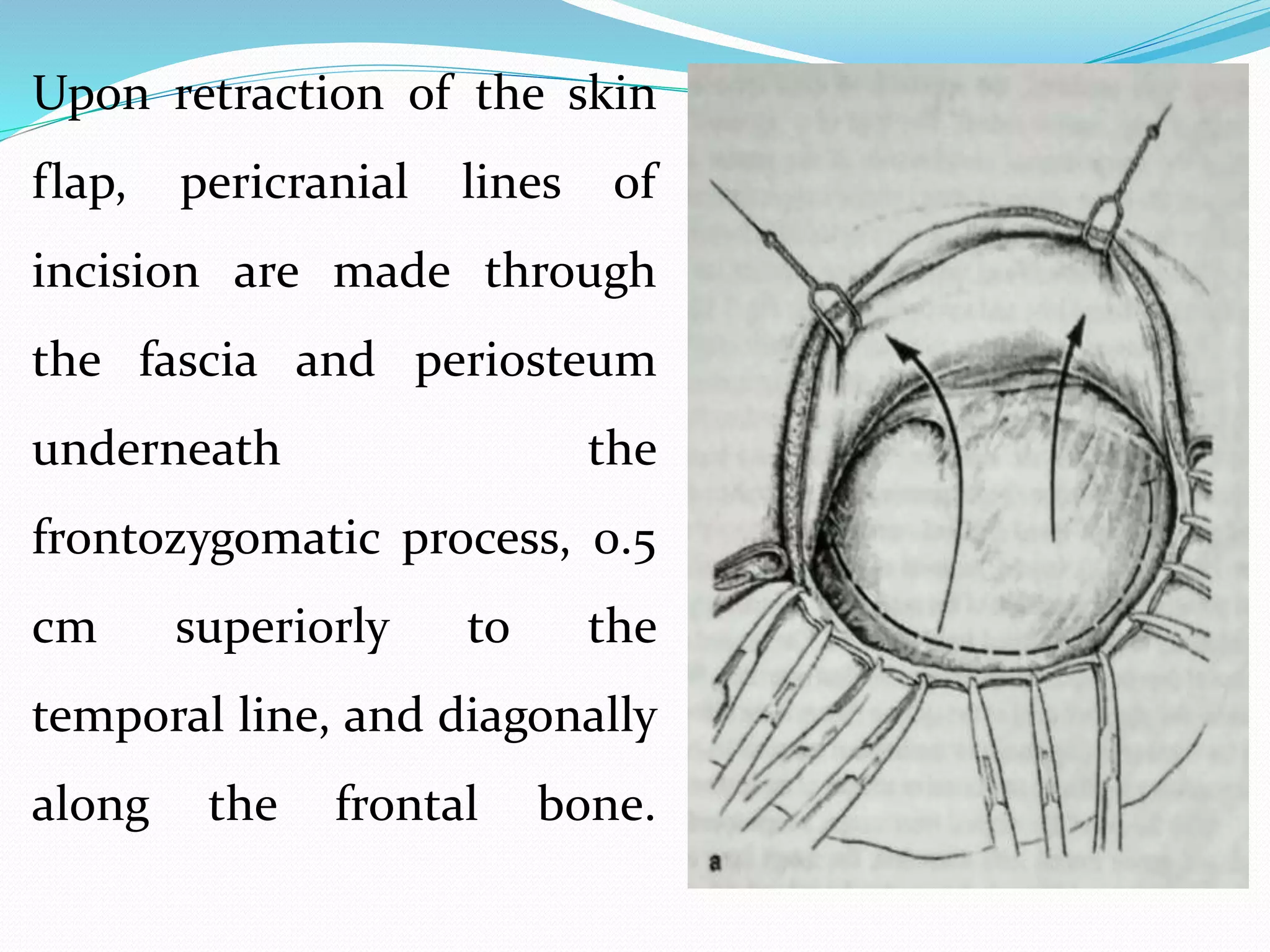
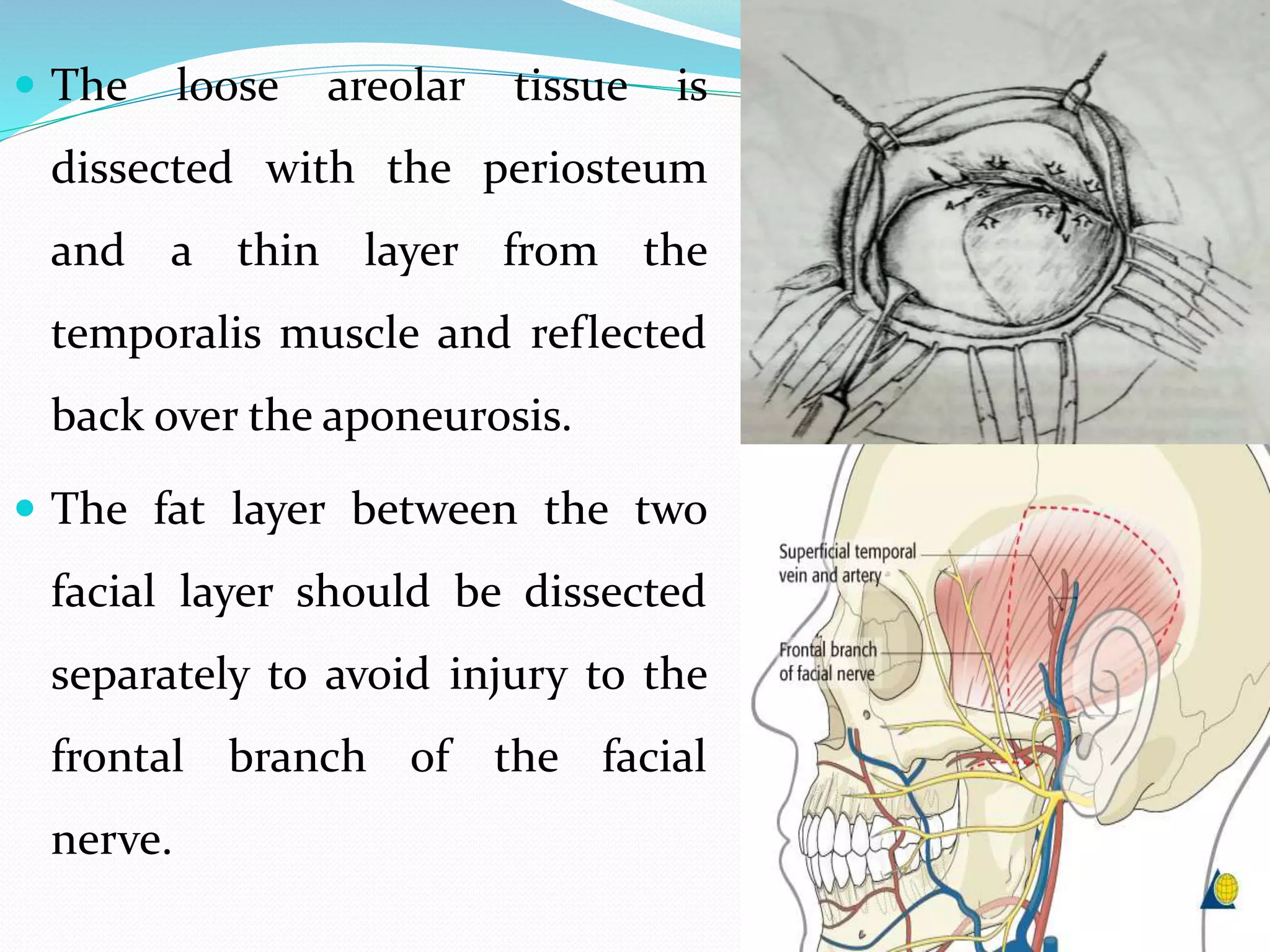
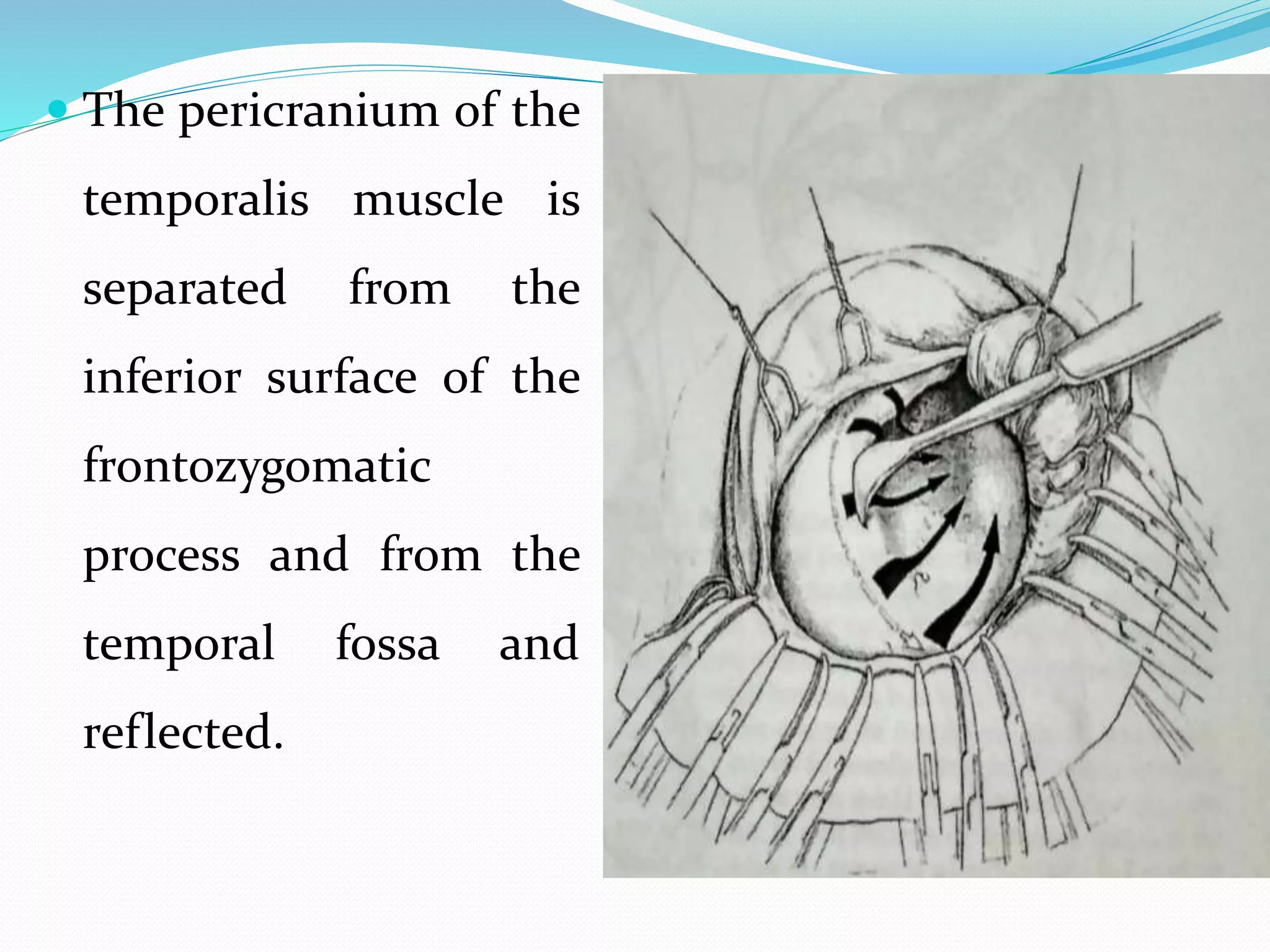
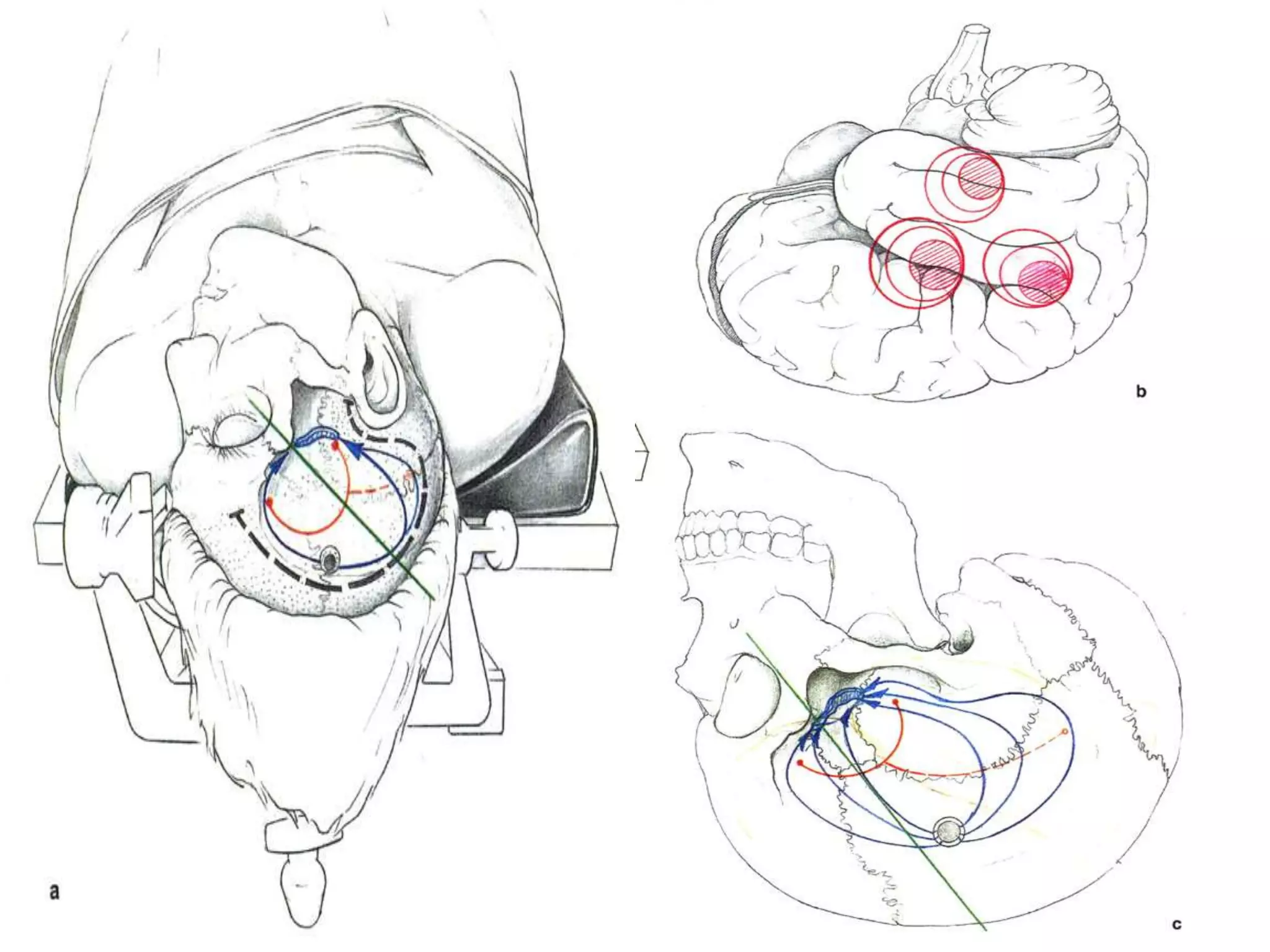
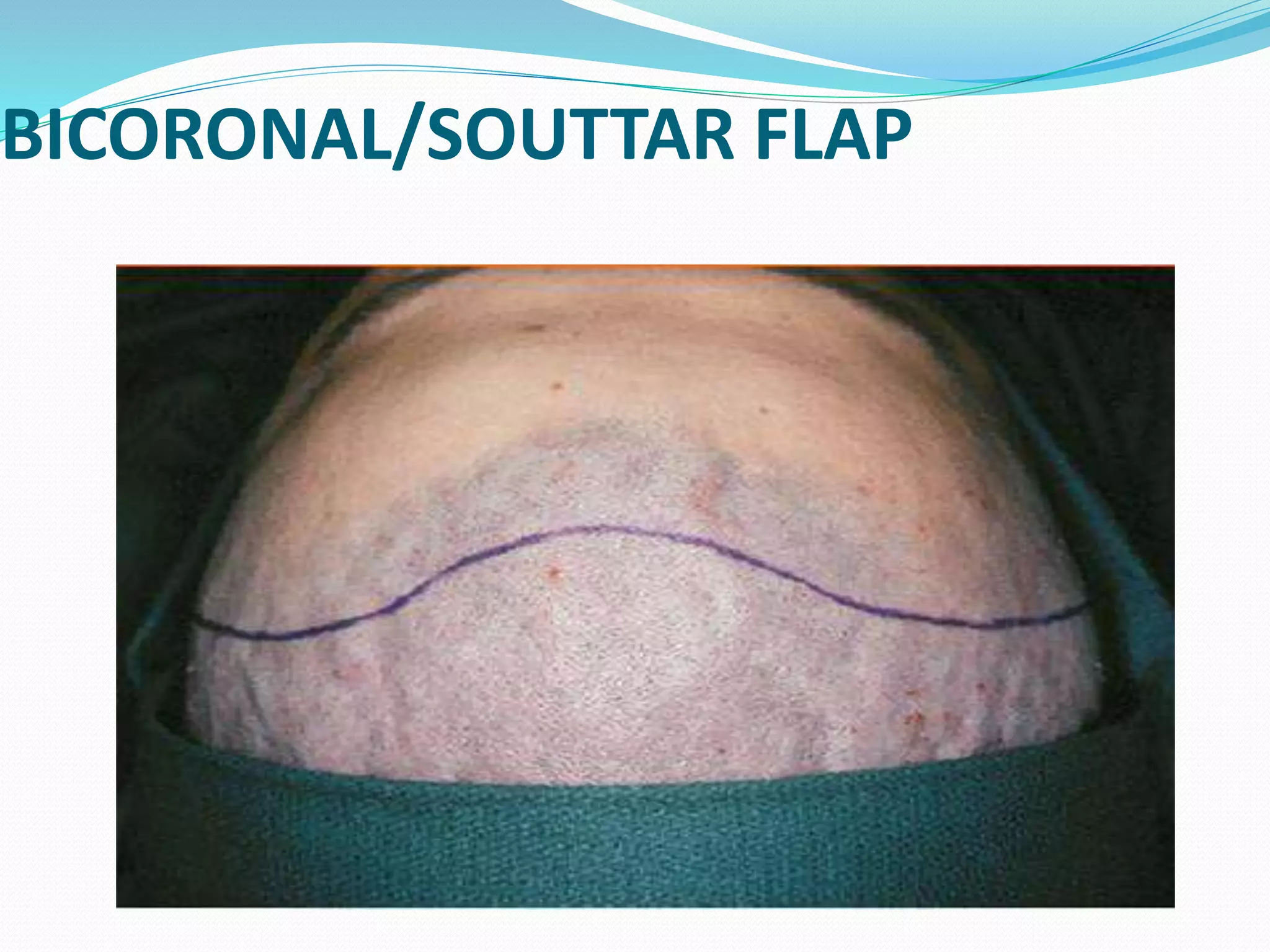
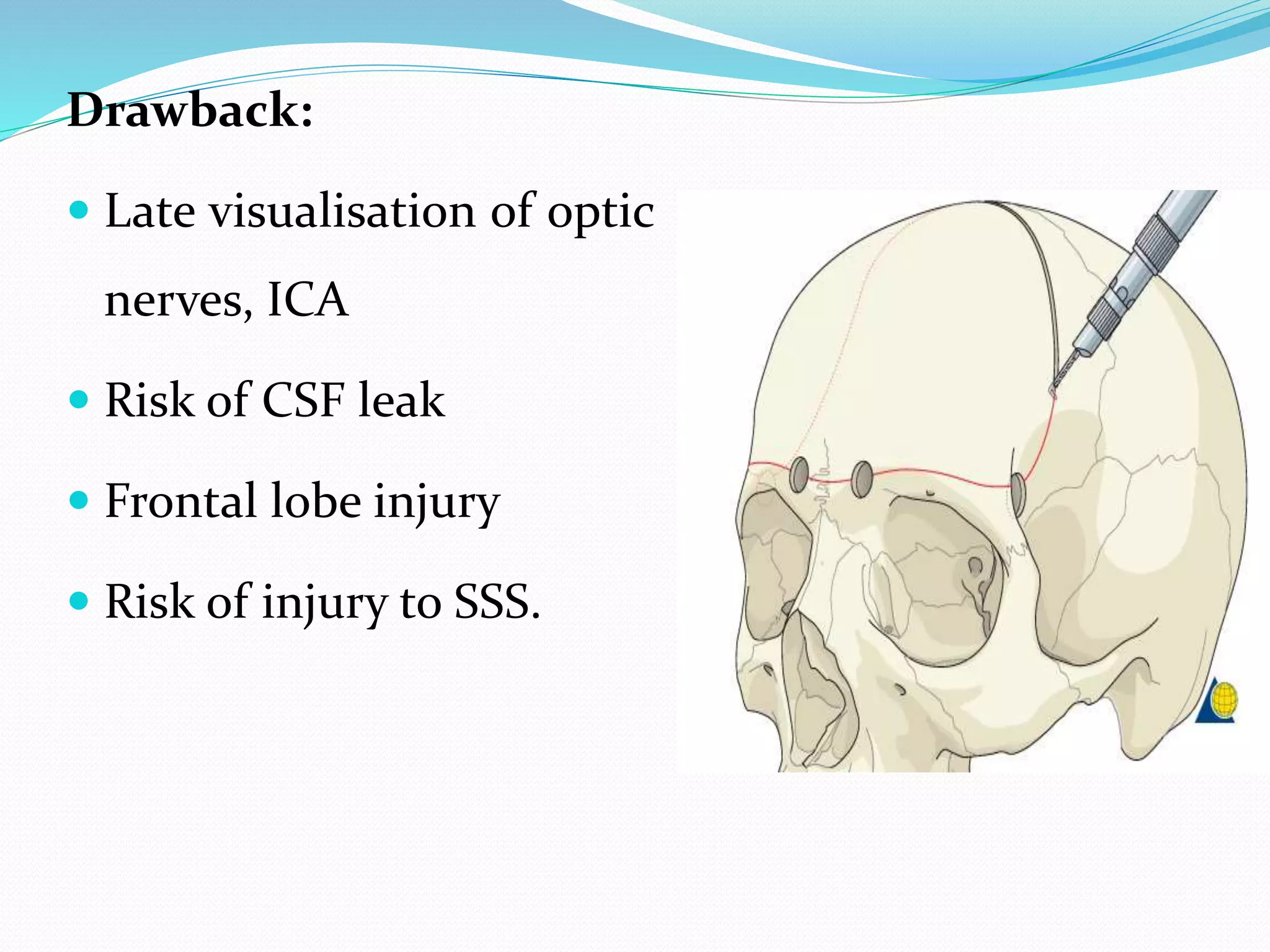
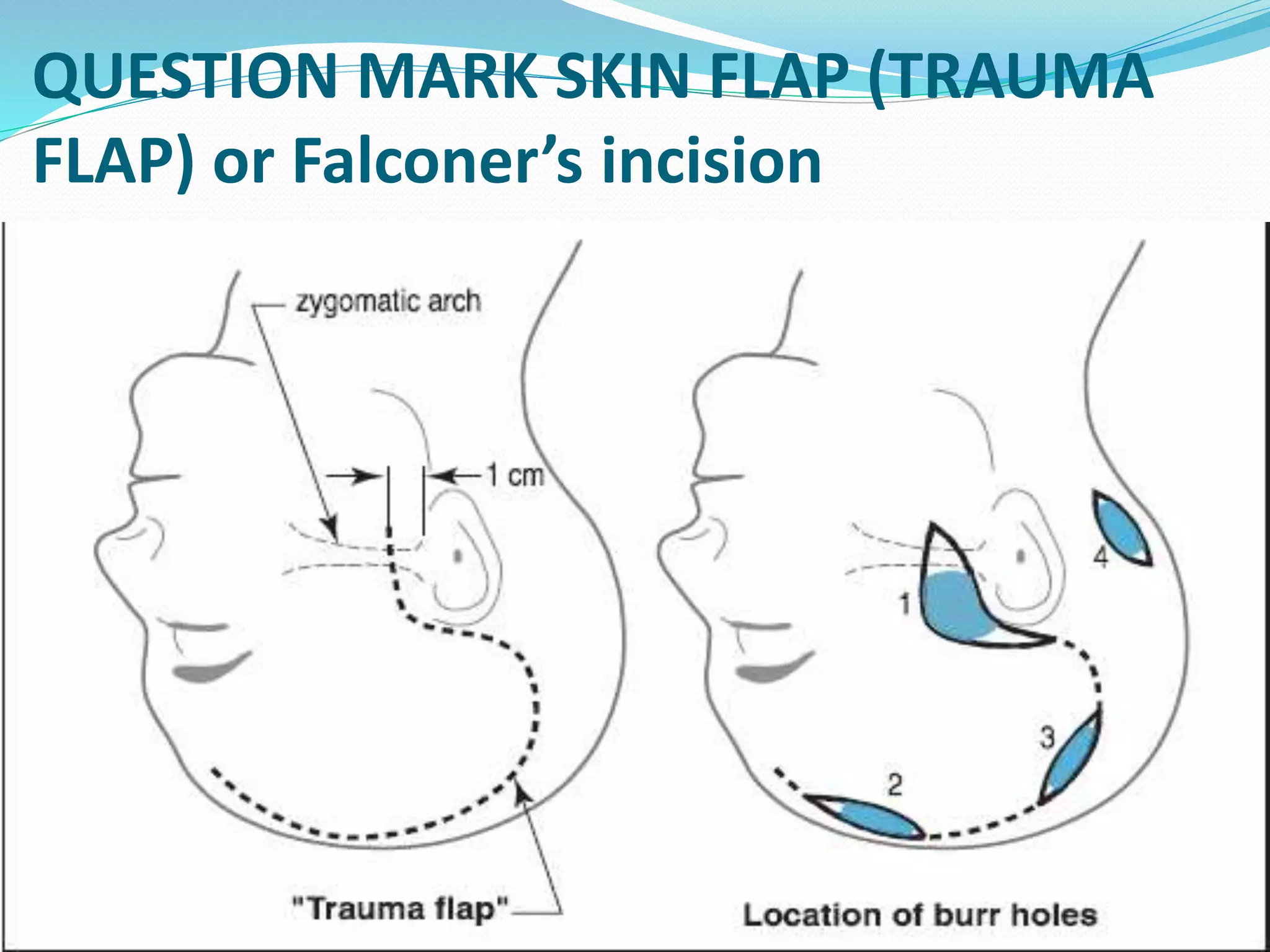
This document provides information on the anatomy and surgical approaches related to the scalp and skull. It describes the layers of the scalp, muscles like the temporalis, nerves like the frontal branch of the facial nerve, and blood vessels. It discusses landmarks and principles for scalp flaps. Various incisions for craniotomies are outlined, including the pterional, bicoronal, question mark, and mitre flaps. Details are provided on procedures like burr holes and craniotomies. Surgical approaches to different brain regions are summarized.