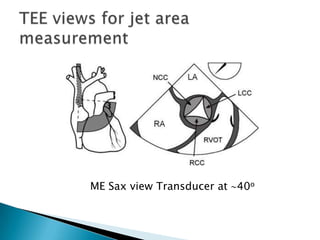
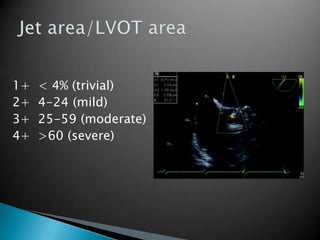
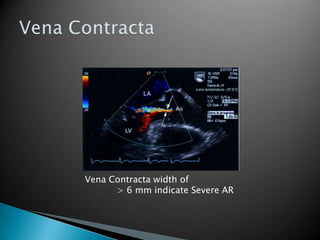
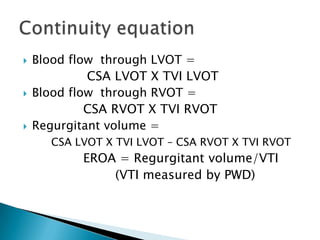
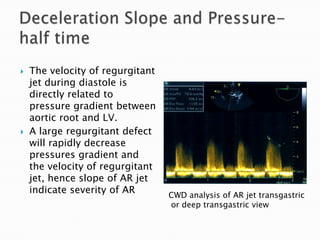
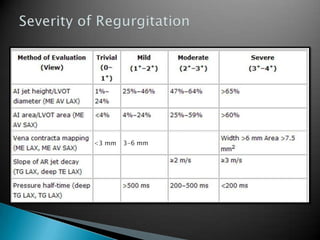
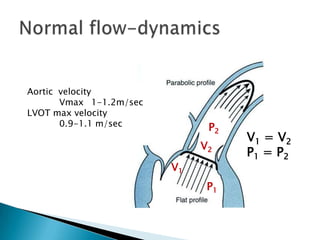
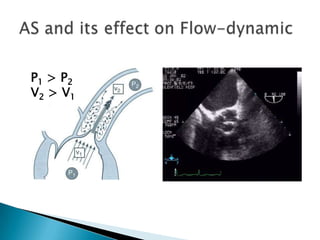
This document discusses techniques for quantifying aortic stenosis and aortic regurgitation using transesophageal echocardiography. It describes using the simplified Bernoulli equation and continuity equation to calculate pressure gradients and regurgitant volumes. Measurement of velocities, pressure half-times, and jet widths are described for assessing severity of aortic regurgitation, while mean and peak gradients help indicate severity of aortic stenosis. Factors like cardiac output and the presence of other valve diseases are also accounted for in the quantification.
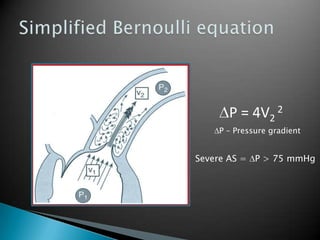
![High CO, similar to low CO, result in over estimation of peak gradient and AS severity.The discrepancy is corrected by measuring the blood flow velocity in the LVOT and applying a correction if the measured LVOT peak velocity exceeds 1.5 m/s. Peak gradient in presence of significant aortic regurgitation = 4 [(peak velocity)2 – (LVOT velocity)2]AS and Aortic regurgitation](https://image.slidesharecdn.com/aorticvalveassessment-110927051333-phpapp02/85/Aortic-valve-assessment-22-320.jpg)