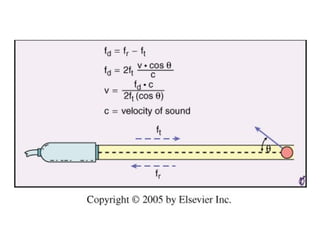
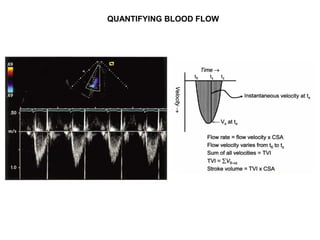
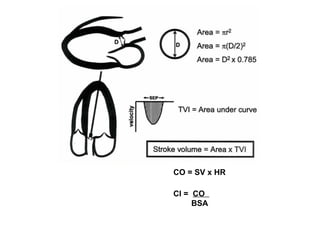
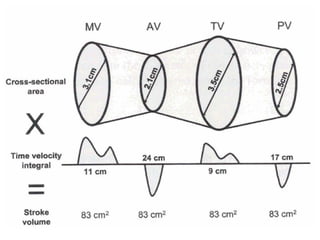
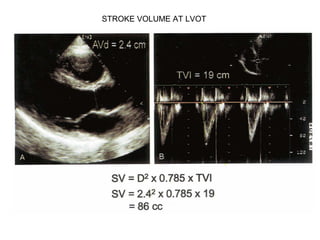
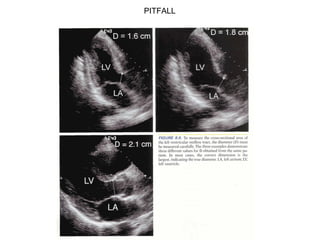
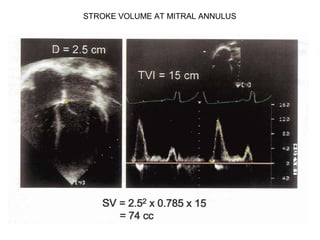
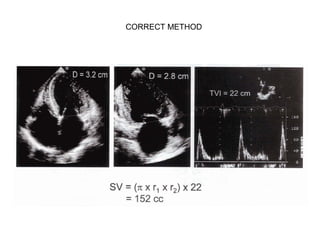
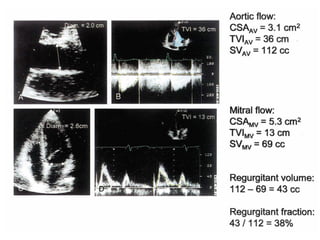
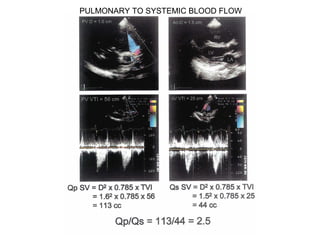
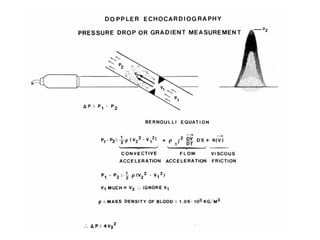
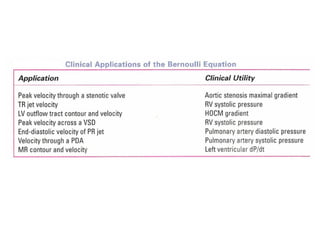
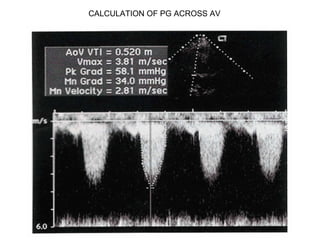
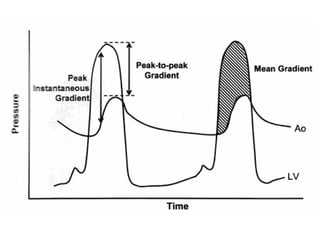
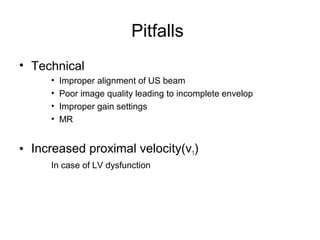
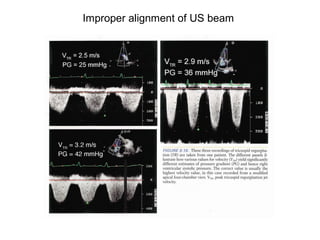
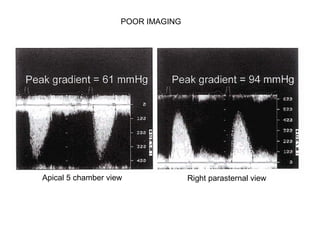
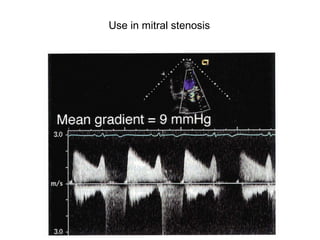
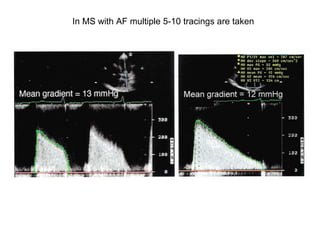
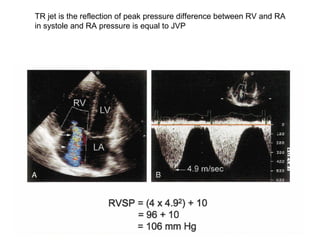
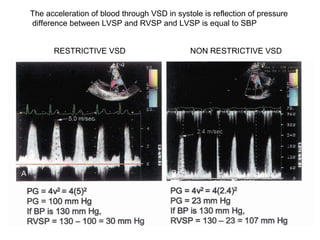
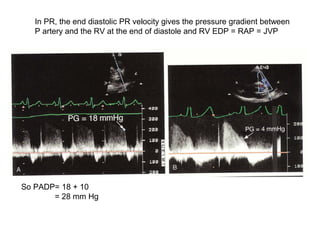
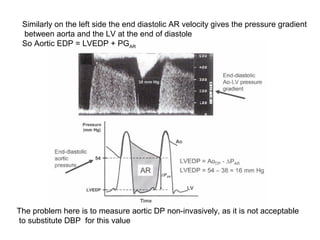
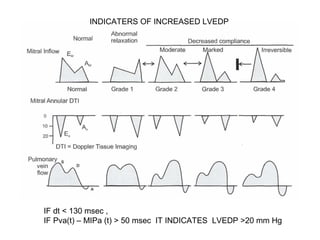
This document discusses hemodynamic assessment using echocardiography. It describes how Doppler shift is used to calculate blood flow velocities and pressure gradients. Methods for quantifying stroke volume at the LV outflow tract and mitral annulus are covered. The use of pulmonary to systemic blood flow ratio and calculation of pressure gradients across valves are explained. Pitfalls related to alignment and imaging quality are addressed. Pressure half-time for assessing mitral stenosis severity is summarized. The document also discusses indicators of increased left ventricular end-diastolic pressure.



































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)

