Downloaded 16 times

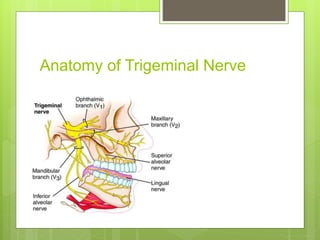

Trigeminal neuralgia is characterized by intense, unilateral facial pain and is primarily idiopathic, but can also result from vascular compression or tumors. Diagnosis is clinical, with consideration for secondary causes through MRI if indicated. Treatment options include carbamazepine, oxcarbazepine, and various surgical interventions if medical management fails.