Downloaded 410 times


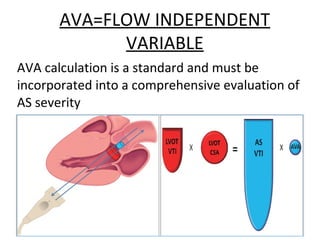

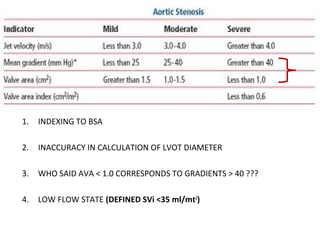
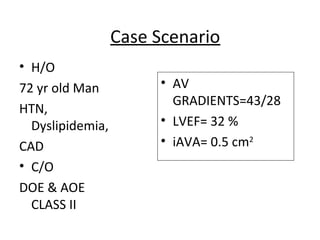
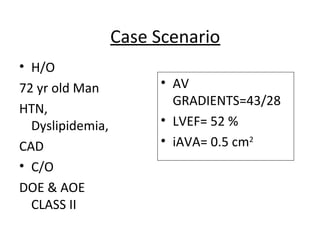
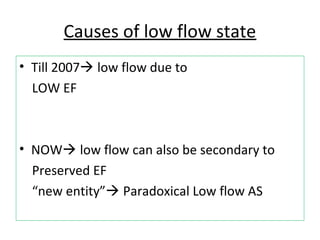
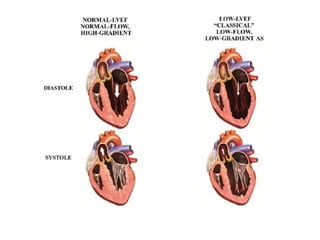




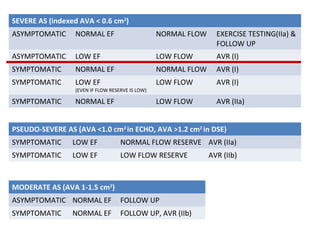

1. Low flow aortic stenosis can be caused by either low or normal ejection fraction and is an important entity that is often underdiagnosed. 2. Evaluation of low flow AS involves calculating aortic valve area using continuity equation in addition to gradients, as well as tests like dobutamine stress echocardiogram, CT calcium scoring, and novel markers of left ventricular function. 3. Treatment depends on symptom status and severity of stenosis, with aortic valve replacement generally recommended for symptomatic patients or asymptomatic patients with low ejection fraction, even in the presence of low flow and gradients.

















































































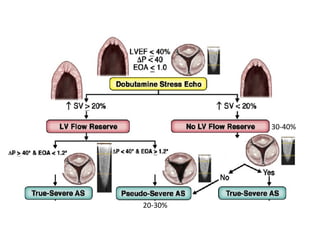
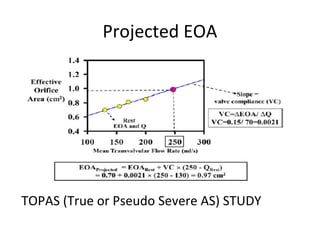
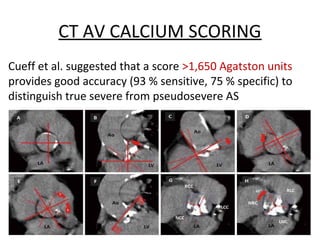
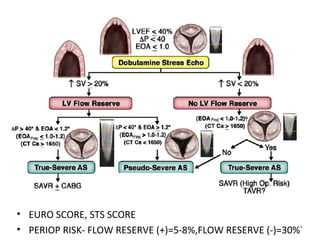
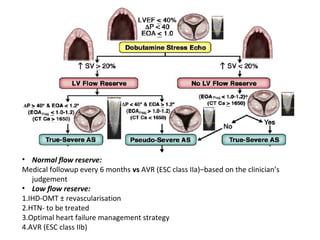
![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)













