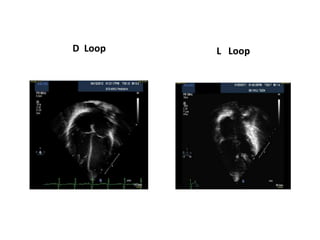
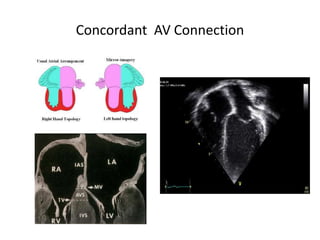
The document describes a segmental approach to describing congenital heart disease. It involves systematically assessing the 3 cardiac segments (atria, ventricles, great vessels) and their connections. Key aspects include determining visceroatrial situs, atrial and ventricular morphology, atrioventricular and ventriculo-arterial connections, and relationships between the great arteries. This approach allows complex CHD to be methodically characterized and expressed segmentally.

























































































![Segmental approach in congenital heart disease [autosaved].pptx 2.pptx final](https://cdn.slidesharecdn.com/ss_thumbnails/segmentalapproachincongenitalheartdiseaseautosaved-141103111700-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)





























