Downloaded 101 times
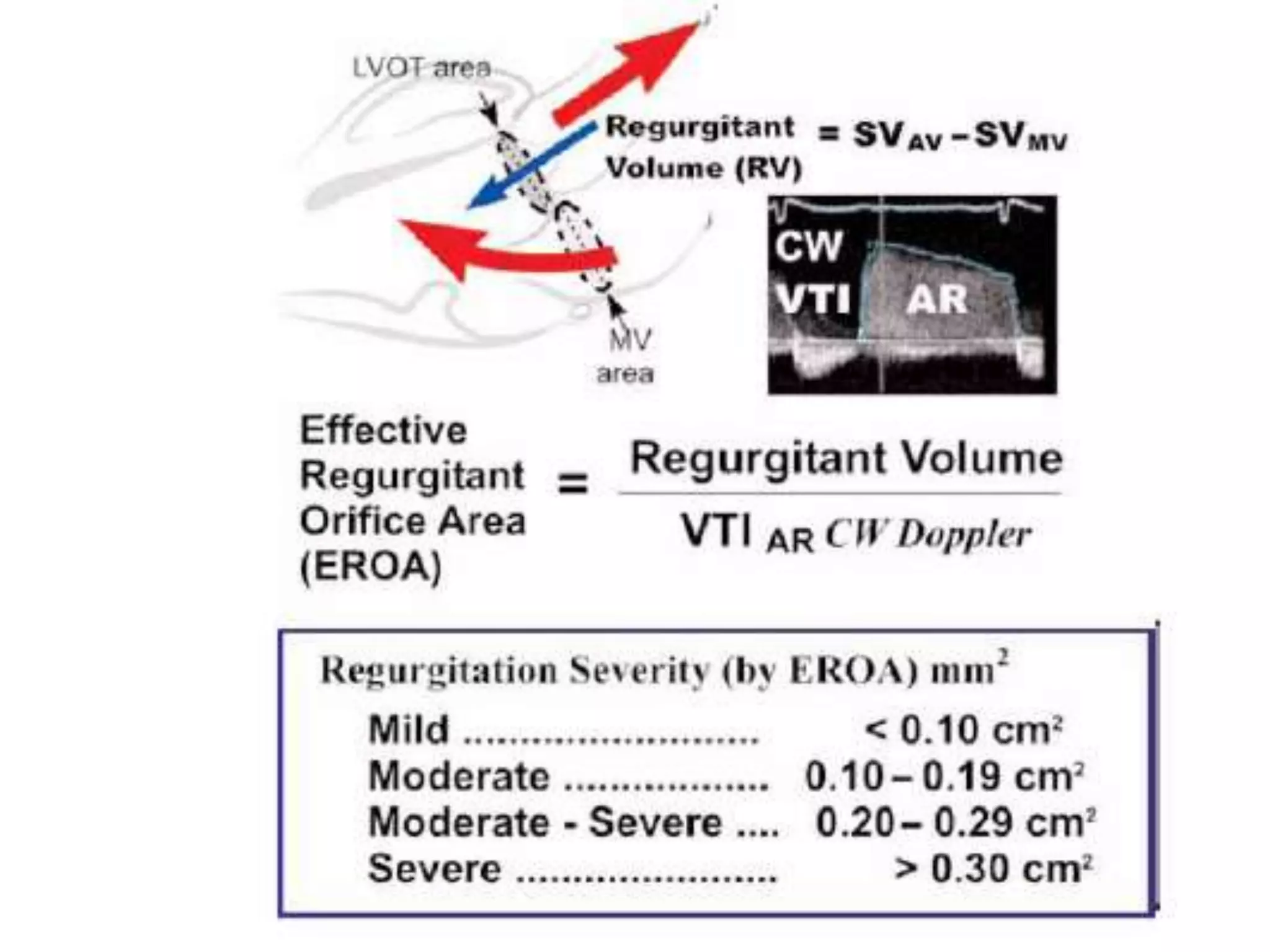
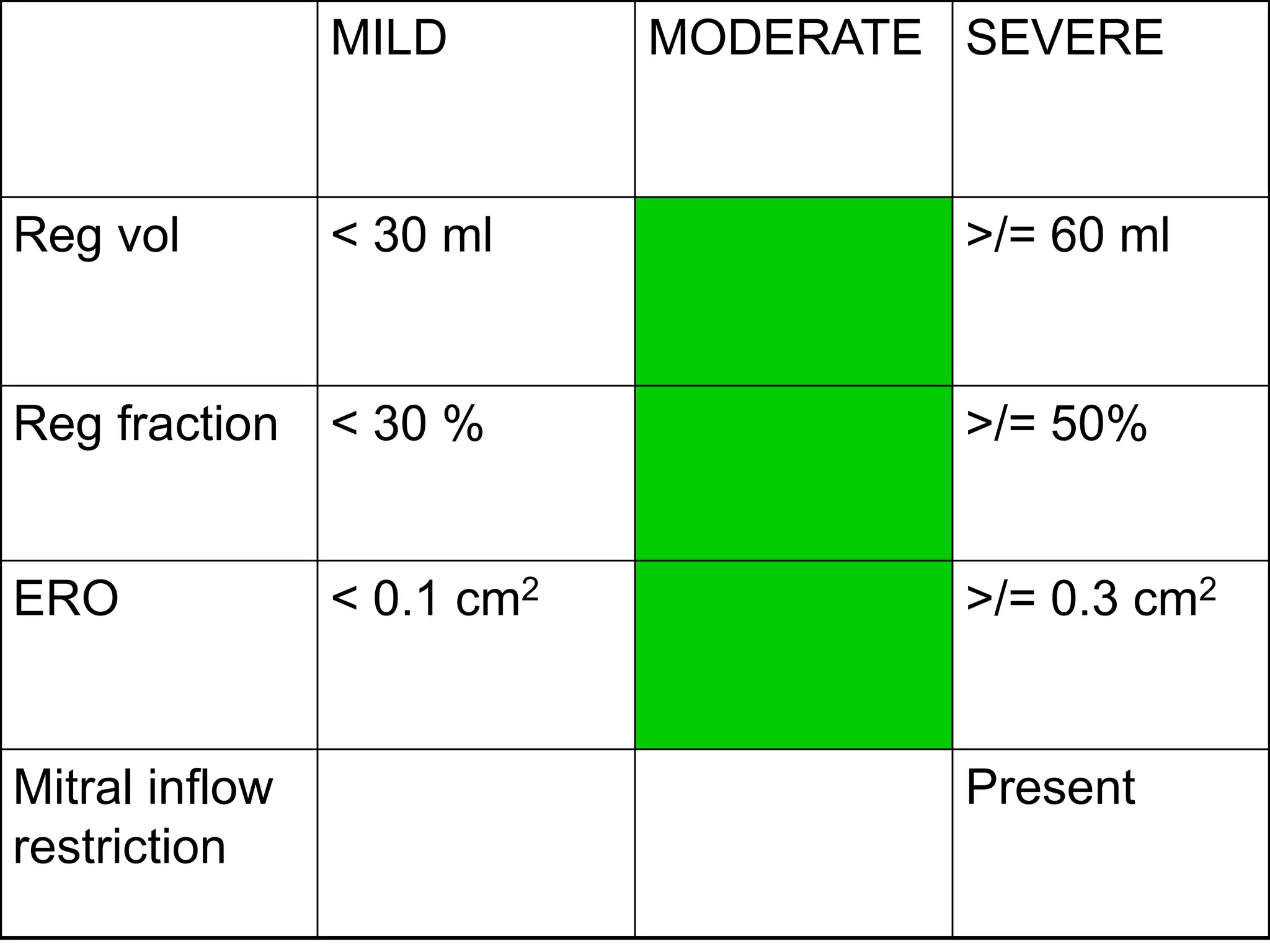
![Calculation of R.Volume and R.fraction
• SV=CSAxVTI
• R.Volume=SV[lvot]-SV[mv]
• RF=R.Volume/SV[lvot]
• ERO=R.Volume/VTI[ARjet]
• R.V>60ml,RF>50%,ERO>0.3cm² indicate severe
AR](https://image.slidesharecdn.com/echoassesmentofasandar-141007093624-conversion-gate02/75/Echo-assesment-of-as-and-ar-87-2048.jpg)


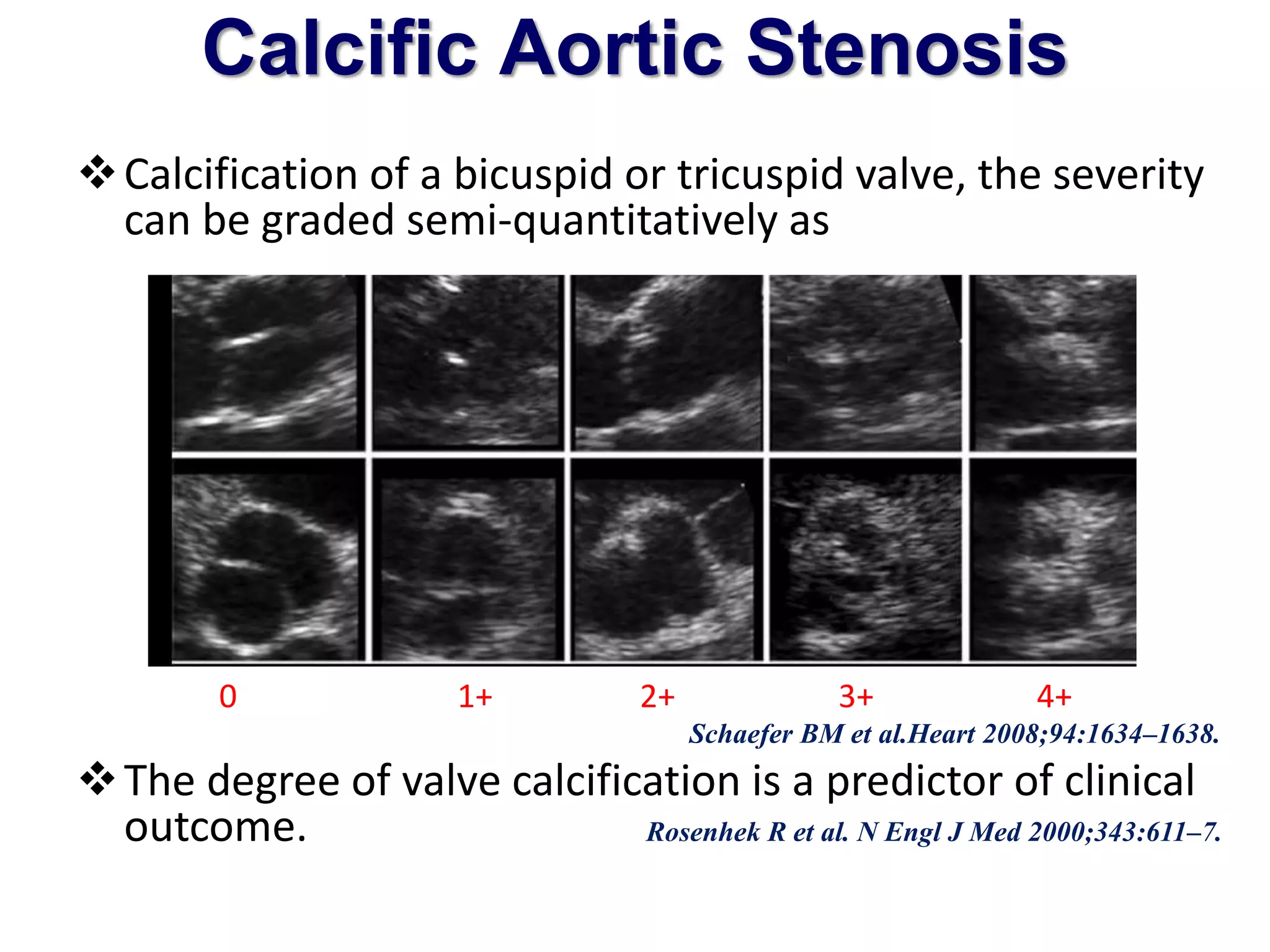
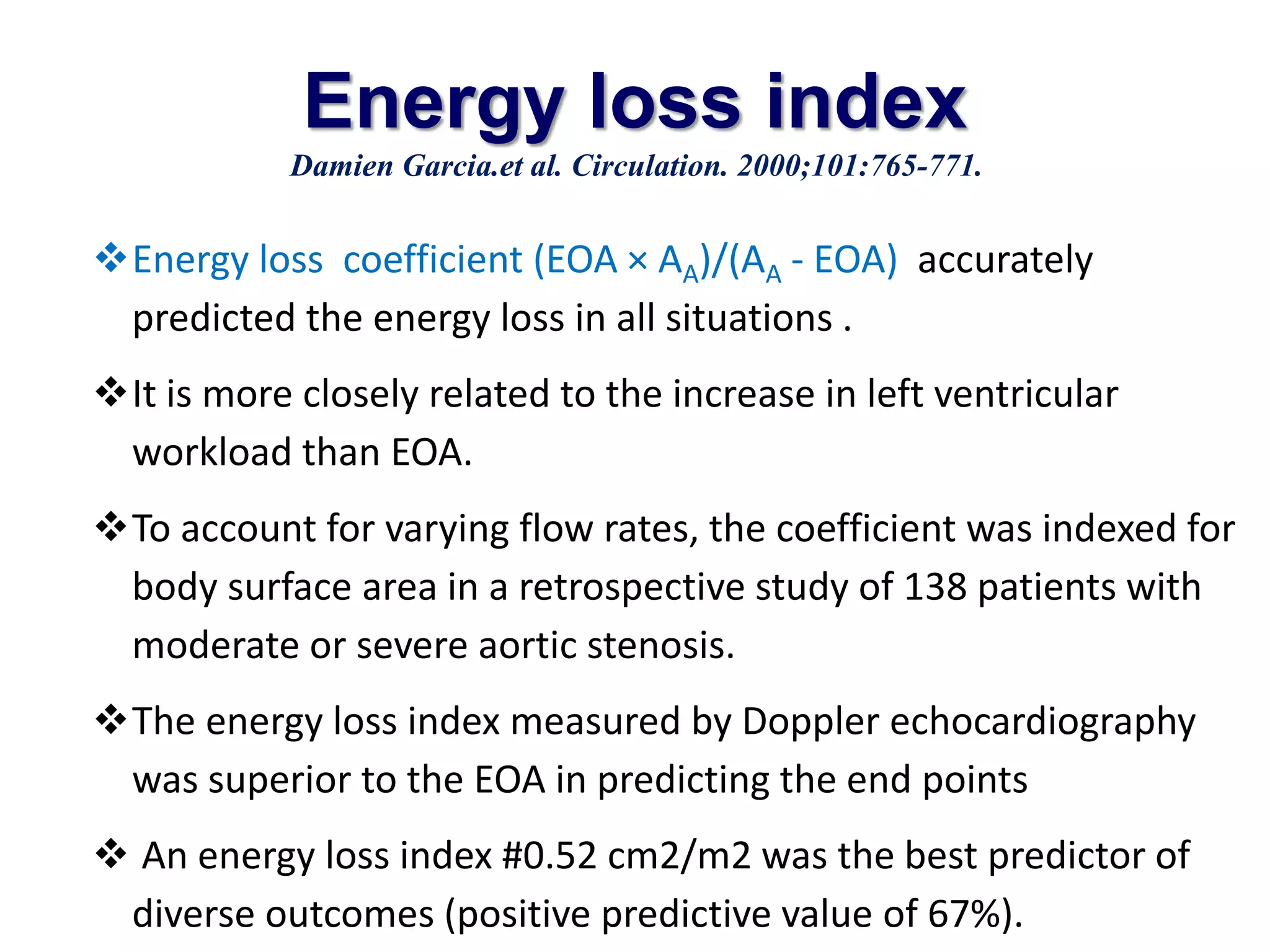
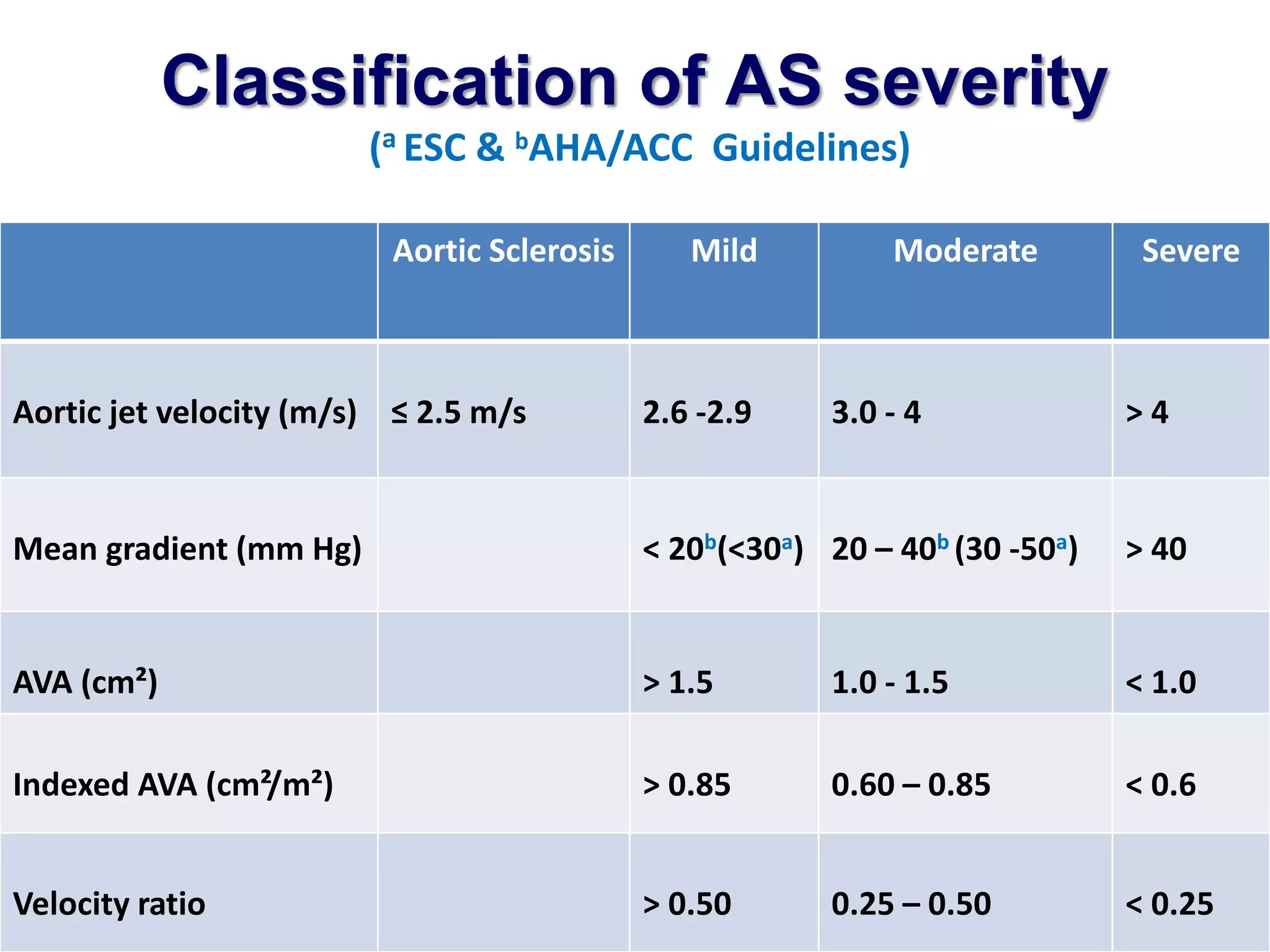
This document discusses the echocardiographic assessment of aortic stenosis and regurgitation. It begins by describing normal aortic valve anatomy and various echocardiographic views used to visualize the aortic valve. It then covers the causes, anatomical presentations, and echocardiographic findings of various types of aortic valve disease including calcific stenosis, bicuspid aortic valve, rheumatic stenosis, and others. The document focuses on Doppler assessment of aortic stenosis, including peak velocity, mean gradient, valve area calculation using the continuity equation, and limitations. It also discusses low-flow low-gradient aortic stenosis and the role of dobutamine stress echocardiography.























































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)


















