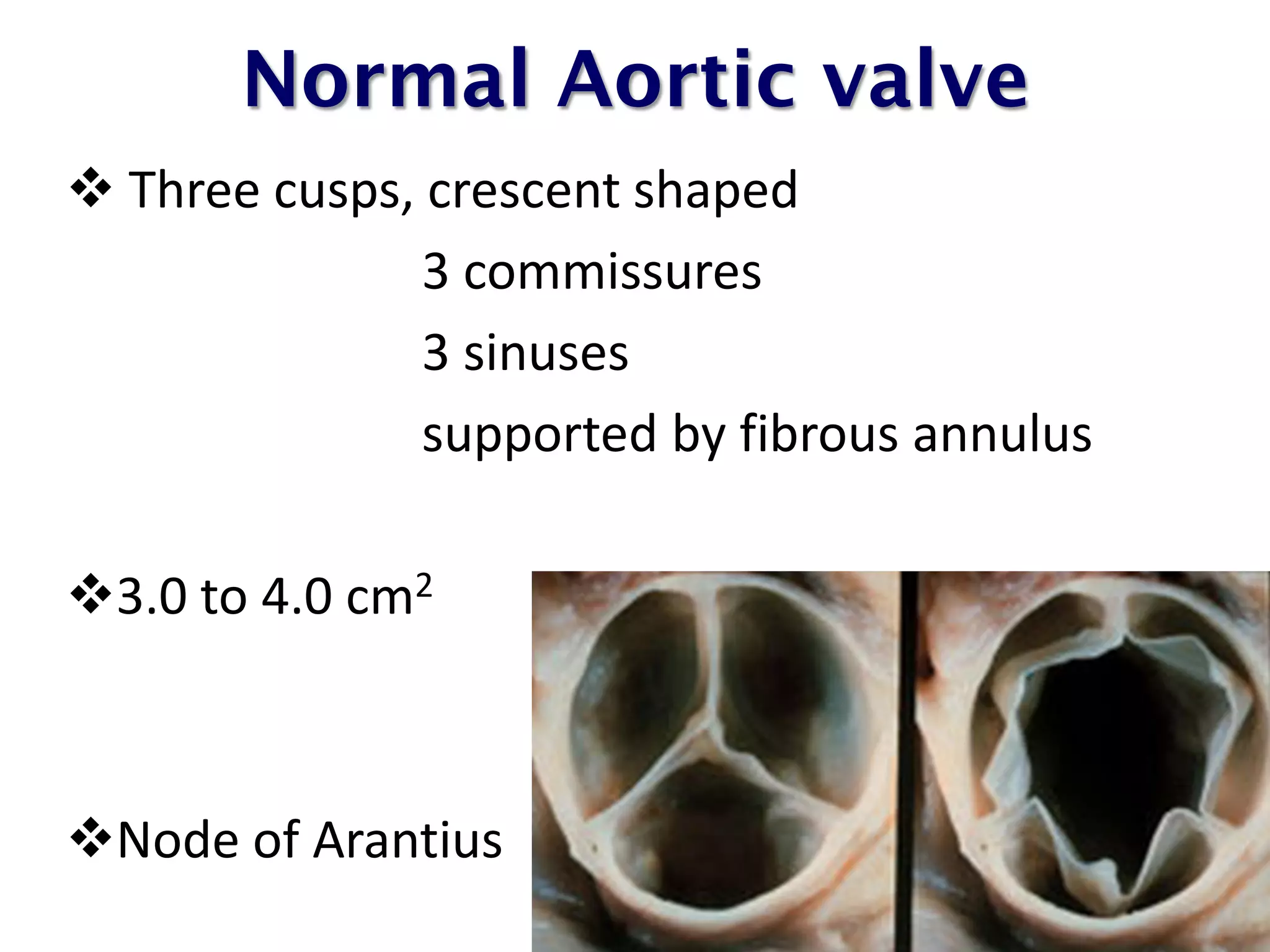
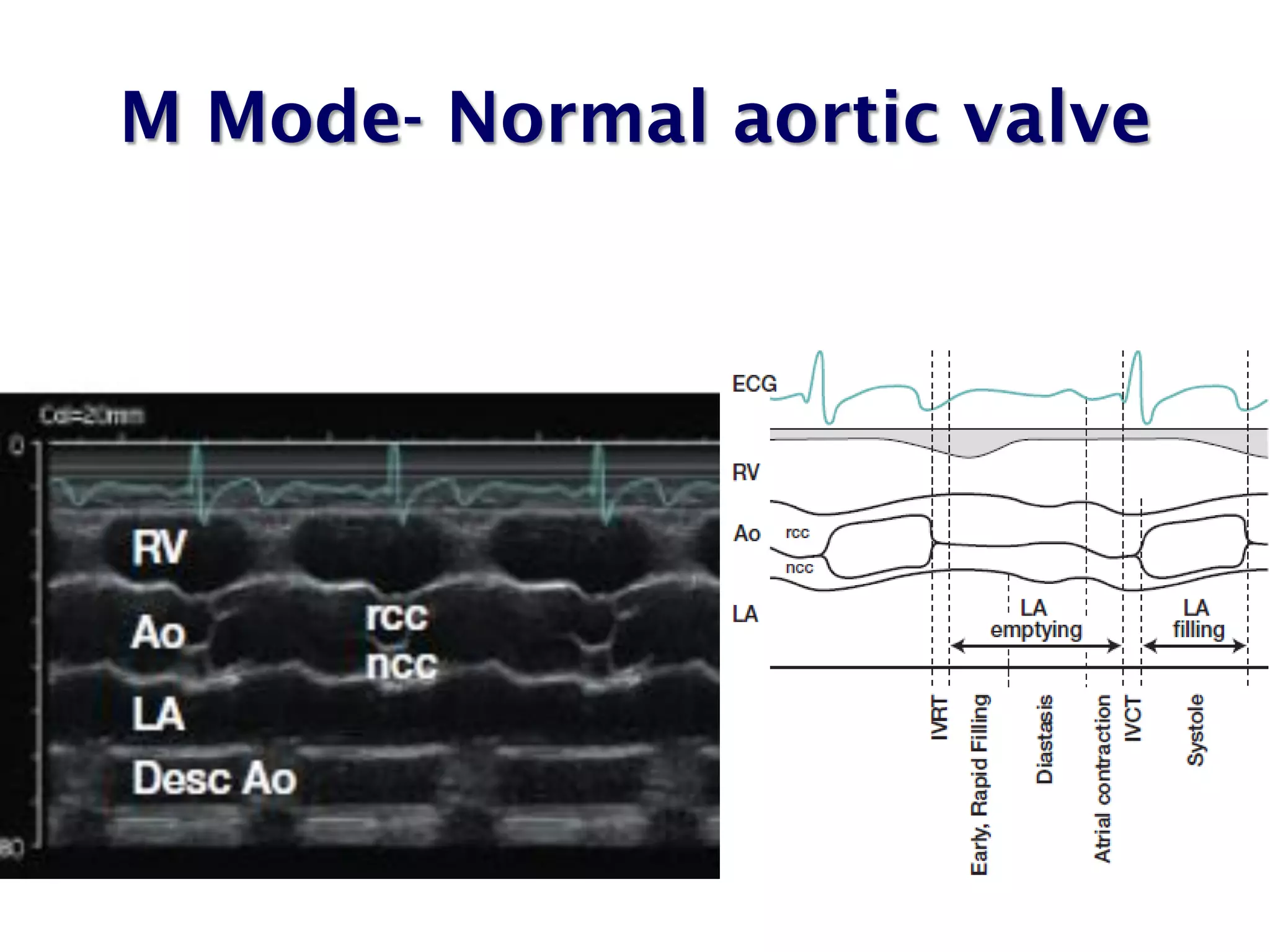
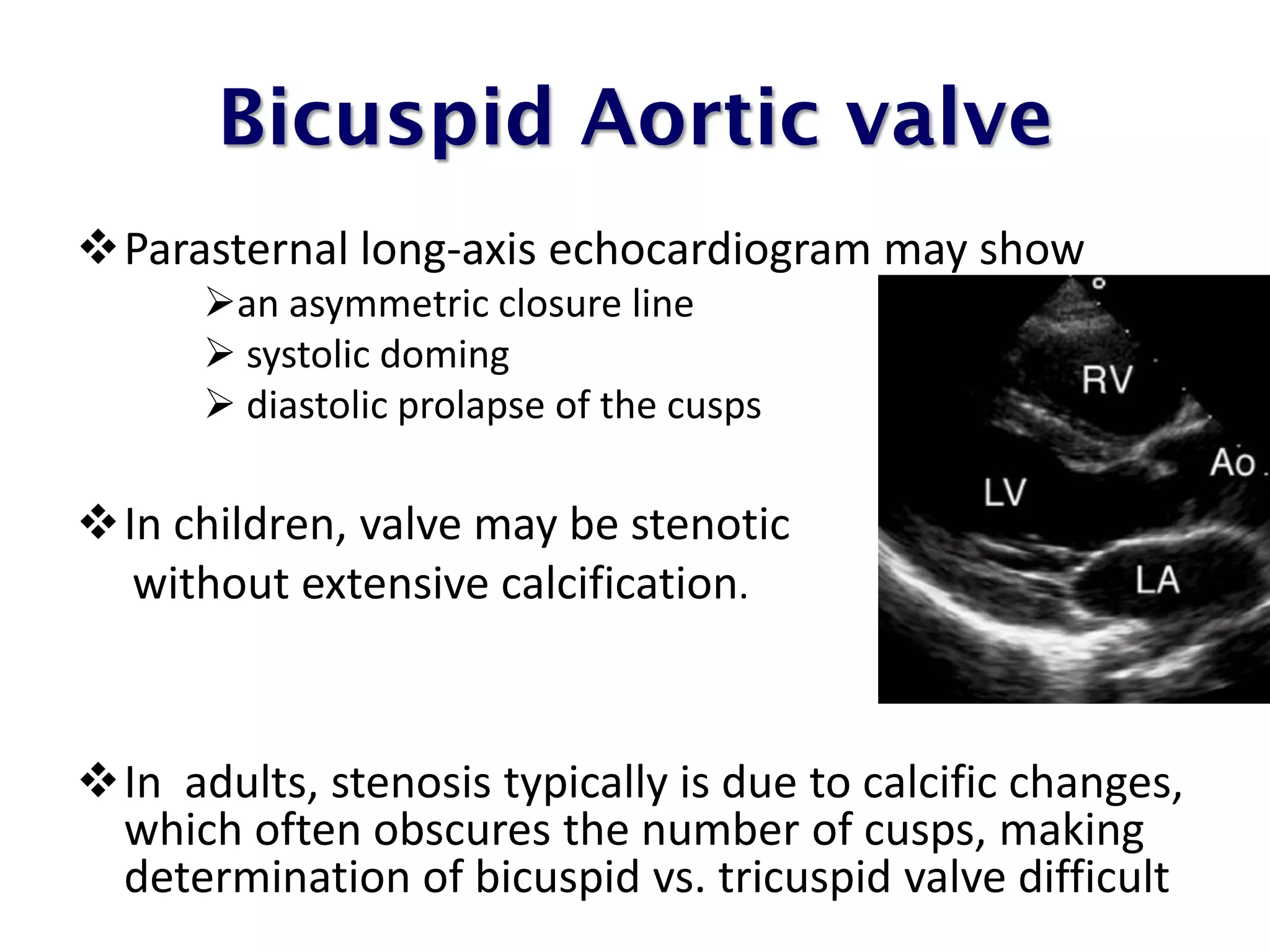
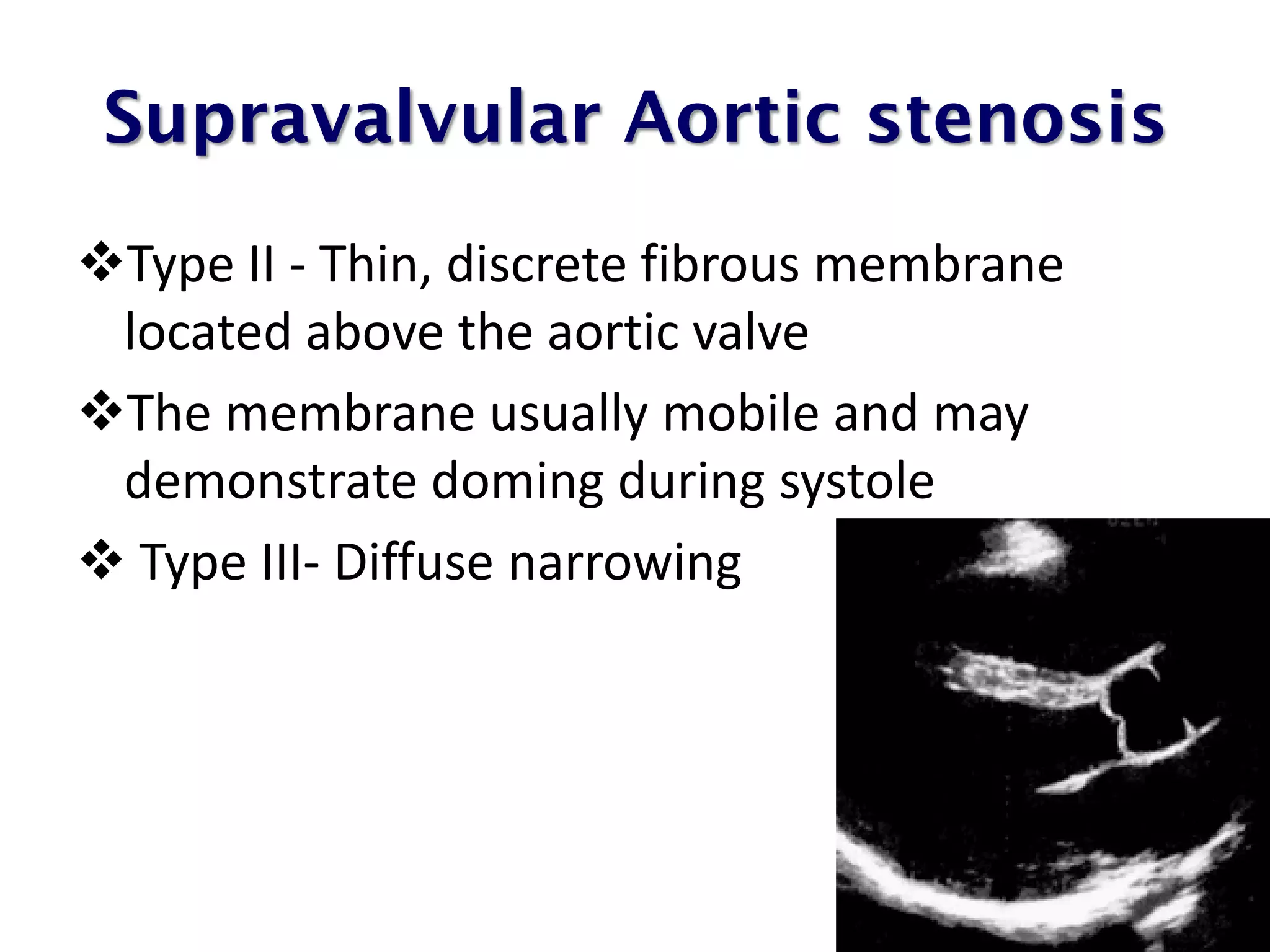
This document discusses the echocardiographic assessment of aortic valve stenosis. It begins by describing the normal aortic valve anatomy. It then discusses various 2D and Doppler echocardiographic views used to evaluate the aortic valve. The main causes of aortic stenosis and their anatomical presentations are described. The key Doppler parameters used to assess stenosis severity are peak aortic jet velocity, mean pressure gradient, and aortic valve area calculated using the continuity equation. Stress echocardiography with dobutamine is discussed for assessing patients with low-flow, low-gradient aortic stenosis. The limitations of echocardiography in evaluating aortic stenosis are also reviewed.