Downloaded 62 times






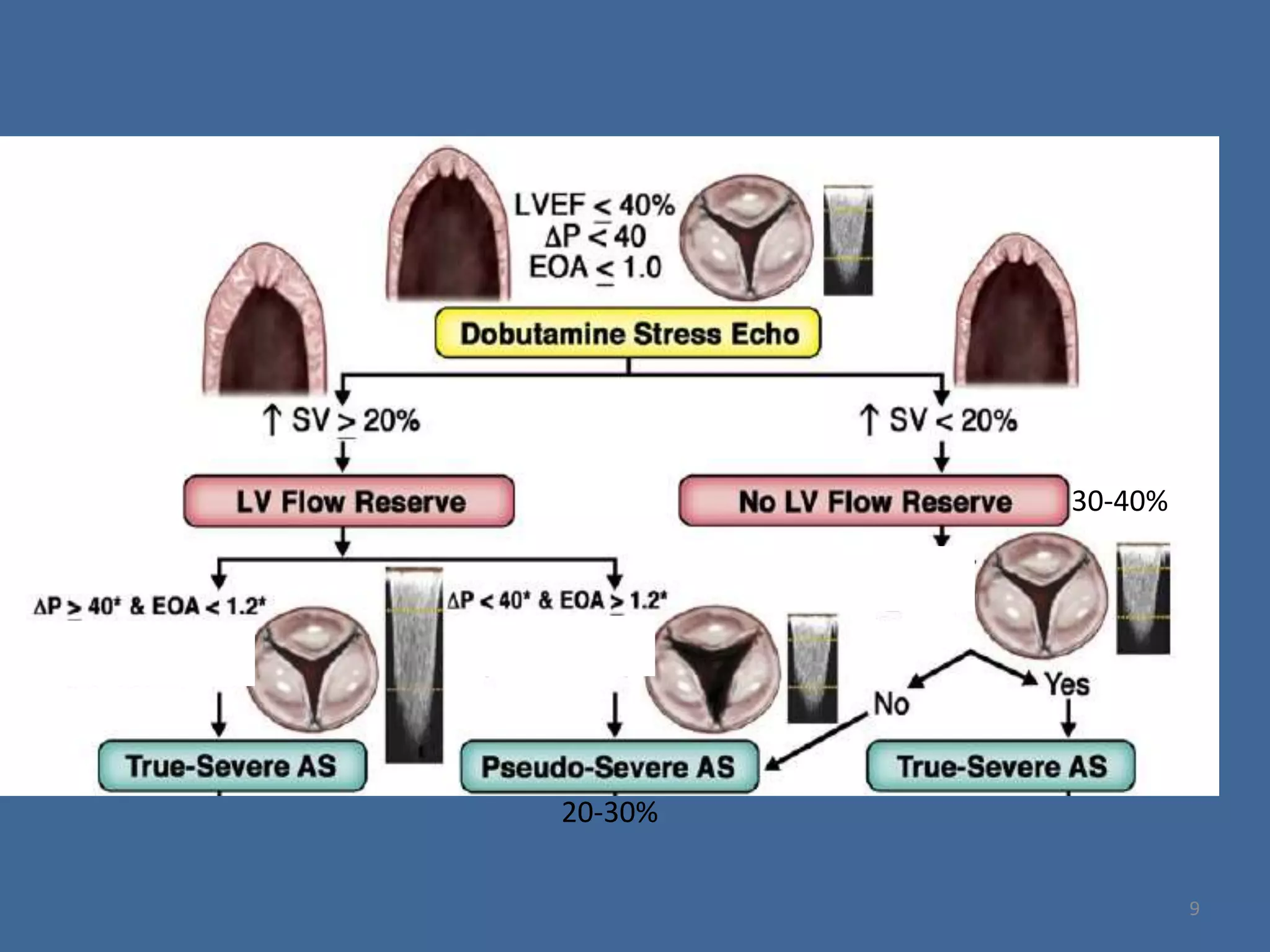




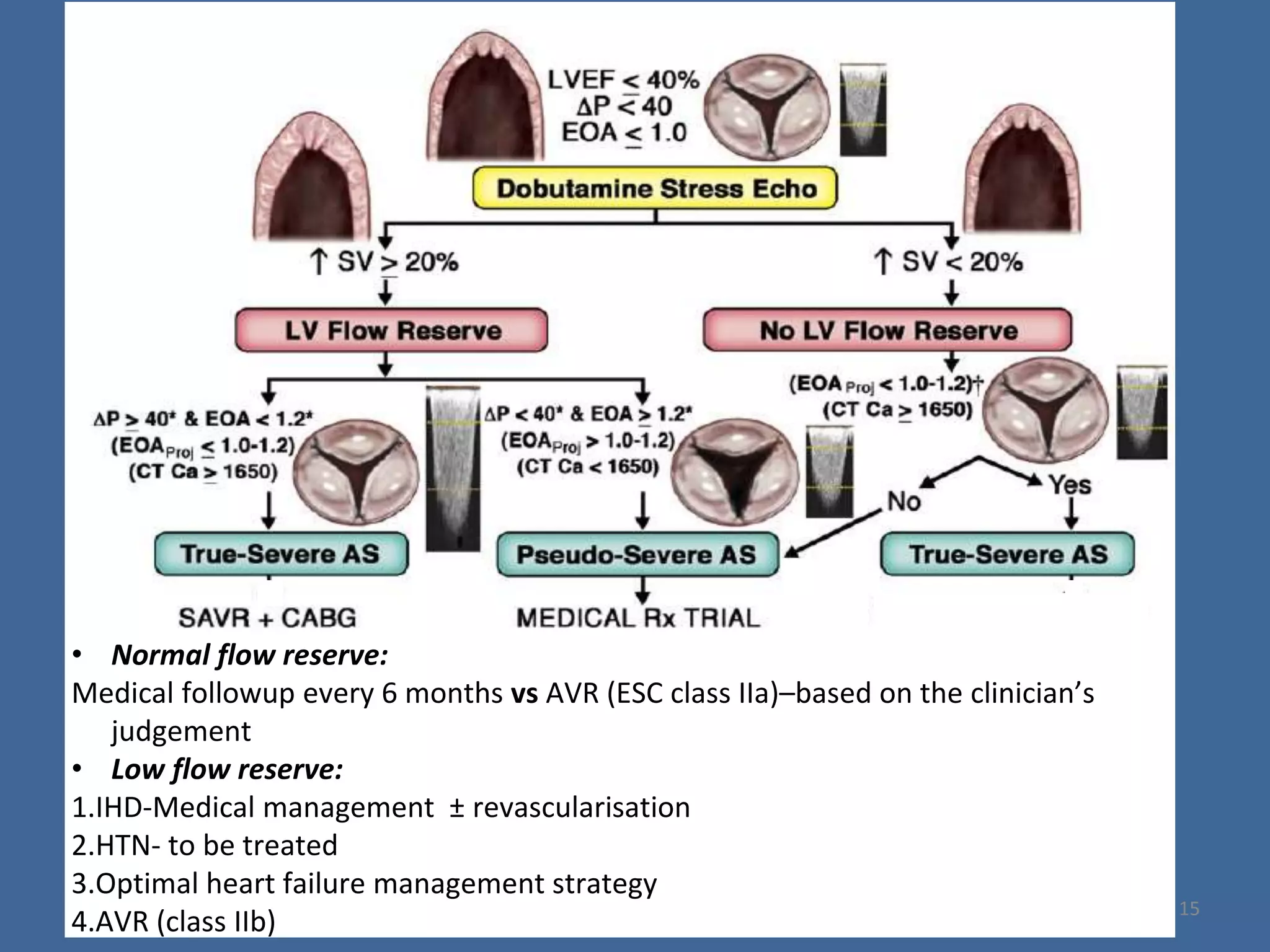











1) Low flow, low gradient severe aortic stenosis can occur with both low and preserved ejection fraction. Dobutamine stress echocardiography is important to differentiate true from pseudo-severe stenosis. 2) For low ejection fraction, aortic valve replacement is recommended irrespective of symptoms or flow reserve. 3) For preserved ejection fraction, alternatives to ejection fraction like valvulo-arterial impedance and global longitudinal strain can help identify intrinsic myocardial dysfunction and predict outcomes. Aortic valve replacement may be better than medical management in these patients.



































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)








