Downloaded 568 times


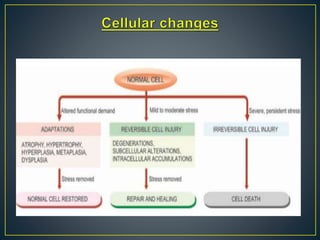
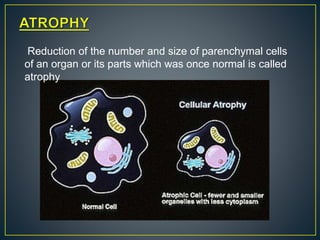
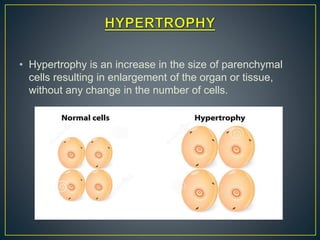
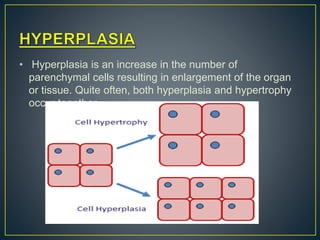

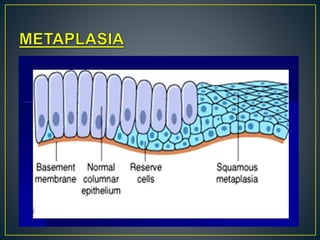


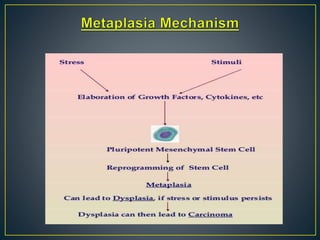
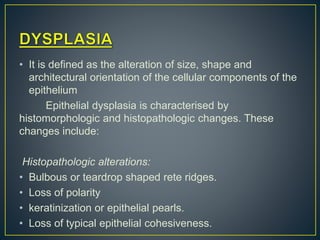
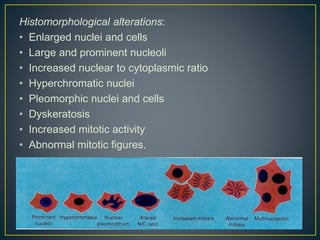





This document discusses various types of cellular adaptations: atrophy, hypertrophy, hyperplasia, metaplasia, dysplasia. Atrophy is a reduction in cell size and number. Hypertrophy is an increase in cell size but not number. Hyperplasia is an increase in cell number. Metaplasia is a change from one adult cell type to another. Dysplasia refers to abnormal cell shapes and sizes that can progress to cancer. Cellular adaptations provide clues for pathologists to diagnose disease.