CELLULAR ADAPTATION
Adaptations arereversible changes in the size, number, phenotype,
metabolic activity, or functions of cells in response to changes in
their environment.
HYPERTROPHY
HYPERPLASIA
ATROPHY
METAPLASIA
2.
HYPERTROPHY
• DEFINATION –Hypertrophy is an increase in the size of cells that results in
an increase in the size of the affected organ.
• TISSUE INVOLVED – Does not have the capacity to divide ( eg Myocardial
Fibres) due to the synthesis and assembly of additional intracellular
structural components.
• High DNA content than normal, because of cell cycle arrest.
• TYPES –Physiological/ Pathological
3.
HYPERTROPHY
• CAUSE -Specific demand or specific hormone stimulation
• PHYSIOLOGICAL HYPERTROPHY- Exercise induced hypertrophy of
muscles- excess load shared by increasd size of the muscle
• PATHOLOGICAL HYPERTROPHY-Left ventricular hyperttrophy in
hypertension, aortic stenosis
• HYPERTOPHY AND HYPERPLASIA OCCURS SIMULTANEOUSLY IN
PREGNANT UTERUS
4.
HYPERTROPHY
• CHANGES INMORPHOLOGY-INCREASE IN MYOFILAMENT
• INCREASE IN SIZE OF INDIVIDUAL CELLS AND ORGAN
• INCREASE IN PROTEIN CONTENT
5.
HYPERTROPHY
MECHANISM INVOVED
1) SIGNALTRANSDUCTION PATHWAYS-
INITIATION OF GENES INVOLVED IN
PROTEIN SYNTHESIS LIKE GF (TGF, IGF),
TRANSCRIPTION GENES (C-FOS, C-JUN)
2) SWITCH OF CONTRACTILE PROTEIN
FROM ADULT TO FOETAL TYPE, ALFA -
MYOSIN REPLACED BY BETA- MYOSIN
TO REDUCE REQUIREMENT OF ATP
3) SOME GENES REEXPRESSED IN
HYPERTROPHY LIKE ANF
Other Factors Involved In Hypertrophy
MECHANICAL STRETCH
TROPIC TRIGGERS LIKE ANGIOTENSIN -
2,ALFA- ADRENERGIC AGONISTS
NUTRIENTS , ENVIRONMENTAL FACTORS
FAILURE OF HYPERTROPHY
6.
HYPERPLASIA
• DEFINATION –Hyperplasia is an increase in the number of cells in an
organ or tissue in response to a stimulus.
• SITE- Any tissue that contains divisible cells
• TYPES - PHYSIOLOGICAL/ PATHOLOGICAL
• PHYSIOLOGICAL HYPERPLASIA – HORMONAL/ COMPENSATORY
7.
PHYSIOLOGICAL HYPERPLASIA
• HOMONALHYPERPLASIA – Happens when functional capacity of
tissue needs to be increasd. Eg- Glandular Epithelial Hyperplasia
in female breast during Puberty and Pregnancy, Muscle Layer
of Pregnant Uterus
• COMPENSATORY HYPERPLASIA -- Partial Resection of Liver Or
Kidney. Bone Marrow cell Hyperplasia in case of acute bleeding
or hemolysis.
8.
MECHANISM OH HYPERPLASIA
PHYSIOLOGICAL--Transcription Of Genes Encoding Growth
Factors, Receptors of GF, Cell Cycle Regulators
Increased Production of Growth Factors And Growth Factor
Receptor, Activation of Certain Intracellular Pathways
Role of Stem Cells Present in Tissue
9.
PATHOLOGICAL HYPERPLASIA
MECHANISM –Excess Hormone Secretion or Growth Factors
Hormone/GF act only on TARGET CELLS
Eg:
Endometrial Hyperplasia due to Hormone imbalance
BHP due to Hormone ANF GF
Gynaecomasta in Male Breast
Bone Marrow Hyperplasia in Anaemia
Epidermal/Ectocervical Hyperplasia (Viral Wart) due to HPV--
Precancerous
10.
ATROPHY
DEFINATION –Atrophy isa reduction in the size of an
organ or tissue due to a decrease in cell size and
number.
Following injury , cell size de cell size decreases,
organ size decreased but survives
Types – Physiological & Pathological
11.
PHYSIOLOGICAL ATROPHY
• InFoetus- T.G Duct, Notocord
• In Childhood- PDA
• In Adults- Tonsil, Thymus, Few Lymph Nodes
12.
PATHOLOGICAL ATROPHY
• DisuseAtrophy , Eg Muscles
• Denervation Atrophy
• Ischaemic Atrophy-Atheroslerosis, Changes In Brain In Old Age
• Inadequate Nutrition – Protein Energy Malnutrition
• Loss Of Endocrine Function –Endometrium, Breast
• Pressure Atrophy-hydronephrosis
• Aging
13.
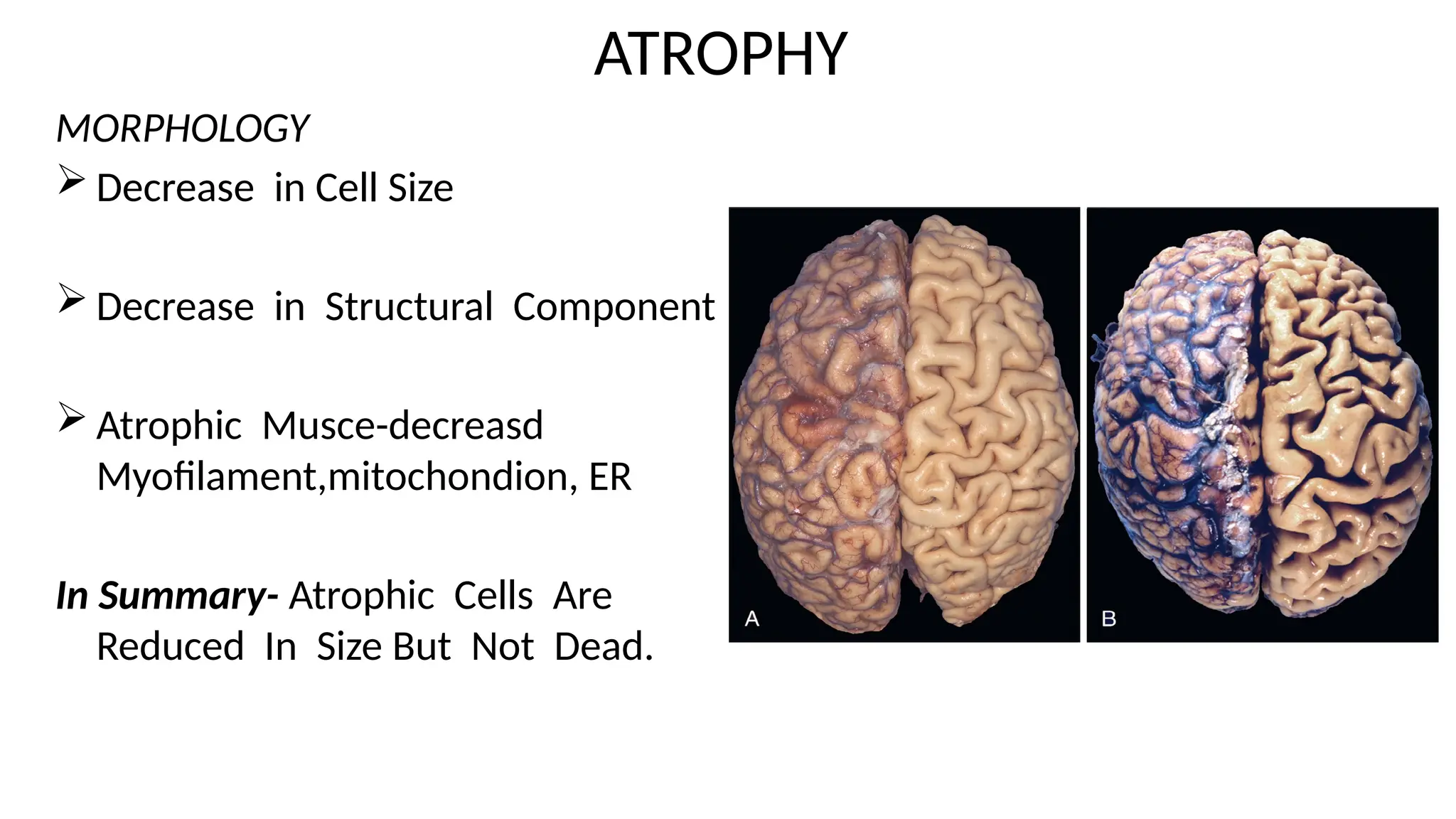
ATROPHY
MORPHOLOGY
Decrease inCell Size
Decrease in Structural Component
Atrophic Musce-decreasd
Myofilament,mitochondion, ER
In Summary- Atrophic Cells Are
Reduced In Size But Not Dead.
14.
ATROPHY
MECHANISM :-- Imbalancebetween Protein Synthesis And Degradation
Breakdown of Protein by :-
1) Lysosome- Destroy endocytose protein, some cell components
2)Ubiquitine-Proteosome Pathway-degrade Cytosol And Nuclear
Protein. Protein Ubiquitine Complex Degrade in Proteosome.
Important in Cancer Cachexia, Muscle Atrophy
15.
METAPLASIA
DEFINATION: Metaplasia isa reversible change in which one
differentiated cell type (epithelial or mesenchymal) is replaced
by another cell type.
OBJECTIVE: Bodies response to external stimuli.
CONSIDERED TO BE AN EARLY PHAGE OF CARCINOGENESIS
DOUBLE AGED SWORD
16.
METAPLASIA
Change due toStress , like Physical or Chemical Irritation
Cells of Origin Still Debatable, may be Stem Cells or Resident
Embryonic Cells.
Other Factors- GF, Cytokines and ECM
Most Common Change -Squamous Metaplasia
DYSPLASIA
DYSPLASIA MEANSDISORDER OF GROWTH
IT IS A PRECANCEROUS CONDITION
IT MAY FOLLOW METAPLASIA BUT CAN ALSO OCCURS INDEPENDENTLY. NOT ALL METAPLASIA DYSPLASTIC
MAINLY FOUND IN EPITHELIUM
CHARACTERISED BY LOSS OF ARCHIETECTURE AND UNIFORMITY OF CELLS.
MITOSIS INCRESED AND MAY PRESENT IN ABNORMAL LOCATION
CIN-1,CIN-2,CIN-3,CIS
UNTREATED PROGRESS TO CARCINOMA